
Tuberculosis in Children — MCQs

A healthcare worker develops fever, night sweats, and cough. Sputum shows acid-fast bacilli. What is the next diagnostic test?
Why is a regimen of four drugs recommended for a TB patient on the first visit?
A patient presents with hemoptysis, weight loss, and fatigue. Chest X-ray shows cavitary lesions in the upper lobes. What is the most likely diagnosis?
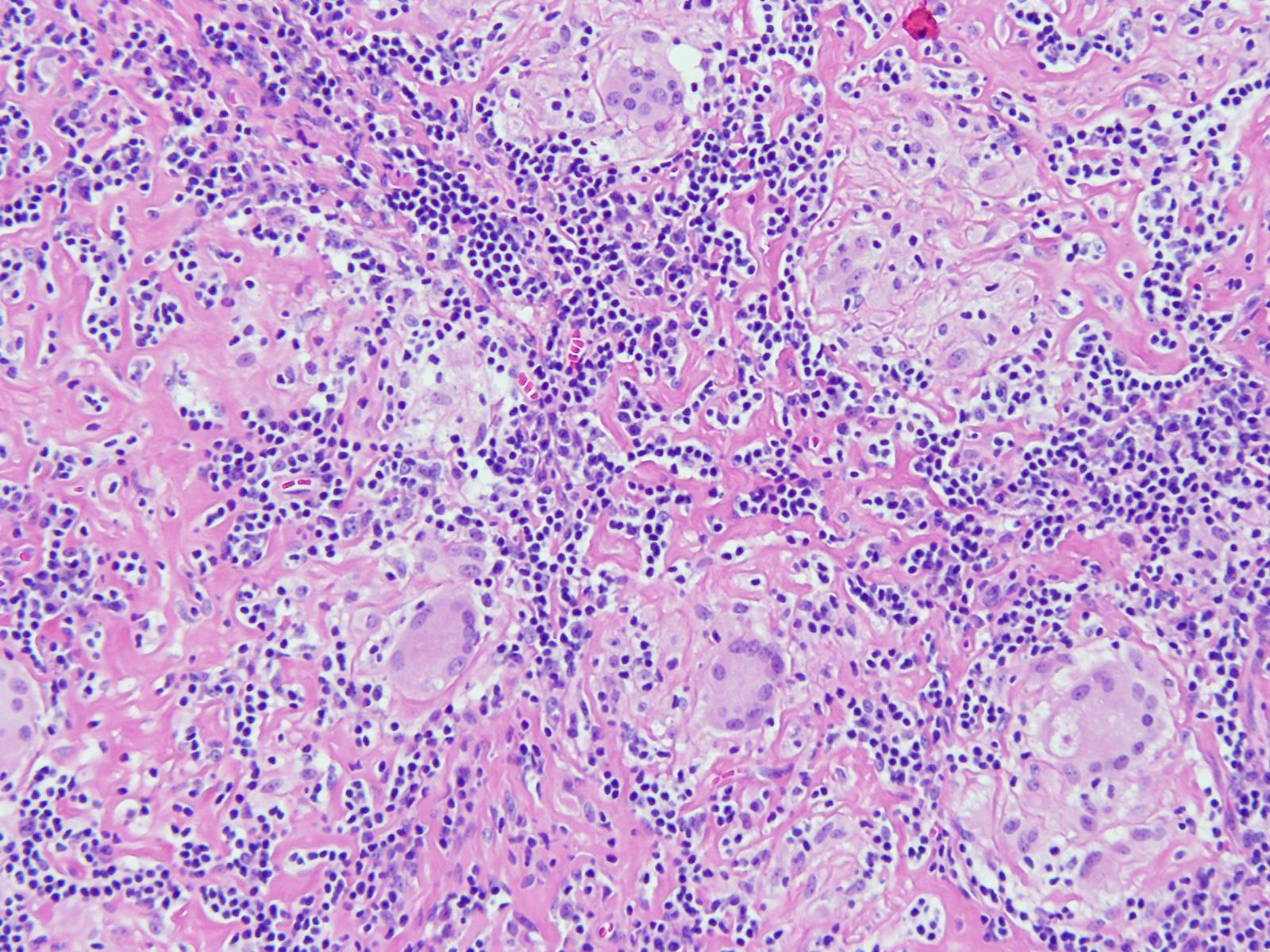
An 11-year-old boy presented with a cough for 15 days. On examination, he was found to have cervical lymphadenopathy. Lymph node biopsy showed the following findings. What could be the diagnosis?
An asymptomatic infant with a history of TB exposure, is 3 months old and had taken 3 months of chemoprophylaxis, what is to be done next?
A poverty-stricken mother suffering from active tuberculosis delivers a baby. Which one of the following would be the most appropriate advice in her case?
A child with acute respiratory distress showing hyperinflation of the unilateral lung in X-ray is due to –
Stridor in an infant is most commonly due to:
Most dangerous sign in lower respiratory tract infection (LRTI) in children is:
A child with recent onset of upper respiratory tract infection after 2 days presents with acute onset of breathlessness, cough, and fever. Which of the following treatments is contraindicated?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app