
Respiratory Diseases — MCQs

On this page
A 2-year-old female child was brought to a PHC with a history of cough and fever for 4 days and inability to drink for the last 12 hours. On examination, the child weighed 5 kg and had a respiratory rate of 45/minute with fever. How would this child be classified?
All of the following statements about cystic fibrosis (CF) are true EXCEPT:
What is the most likely cause of acute onset of cough, stridor, and dyspnea in a child?
Which of the following is the most likely diagnosis in a child presenting with increased cough at night?
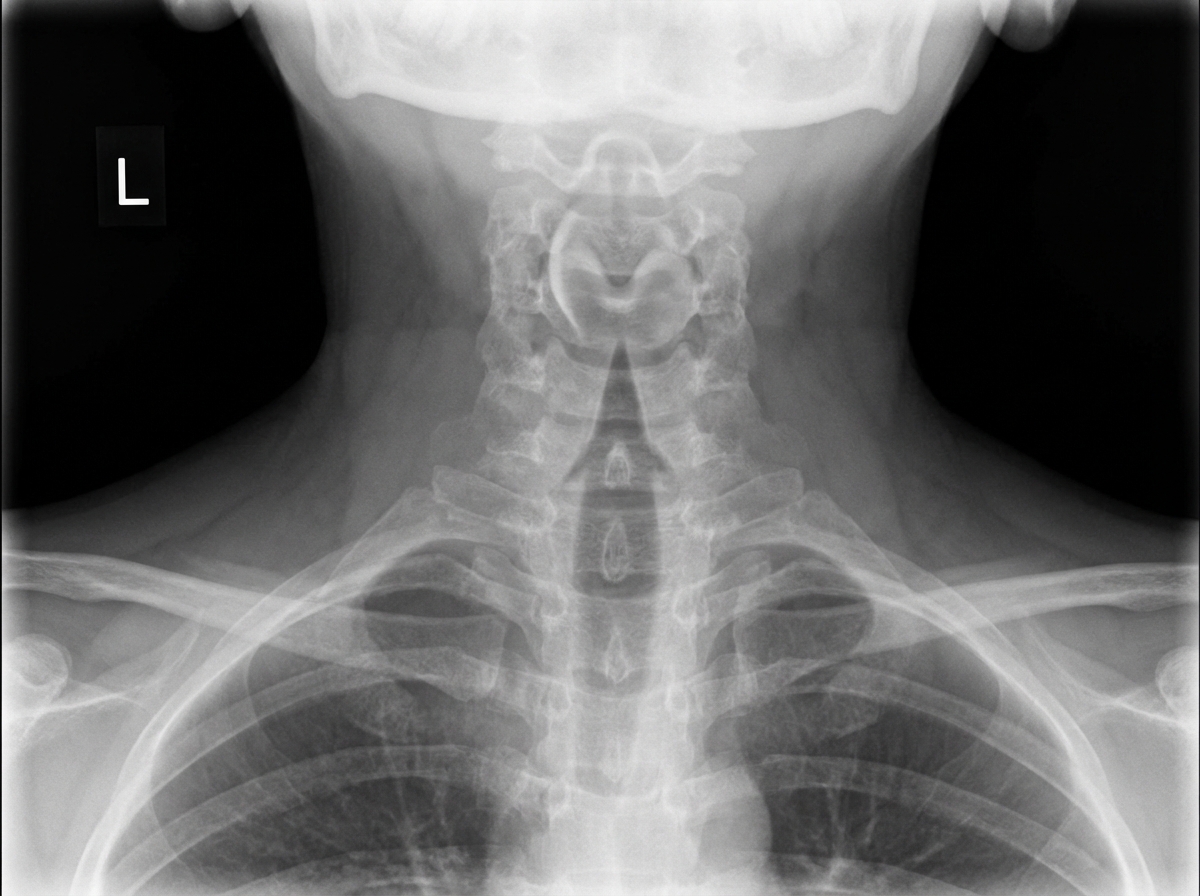
A child presents with fever, stridor, and barking cough. An X-ray is provided below. Which of the following is true about the patient?
Which of the following is FALSE regarding cystic fibrosis?
Which one of the following values is not a feature of acute severe asthma?
Which of the following findings are true about bronchiolitis in children?
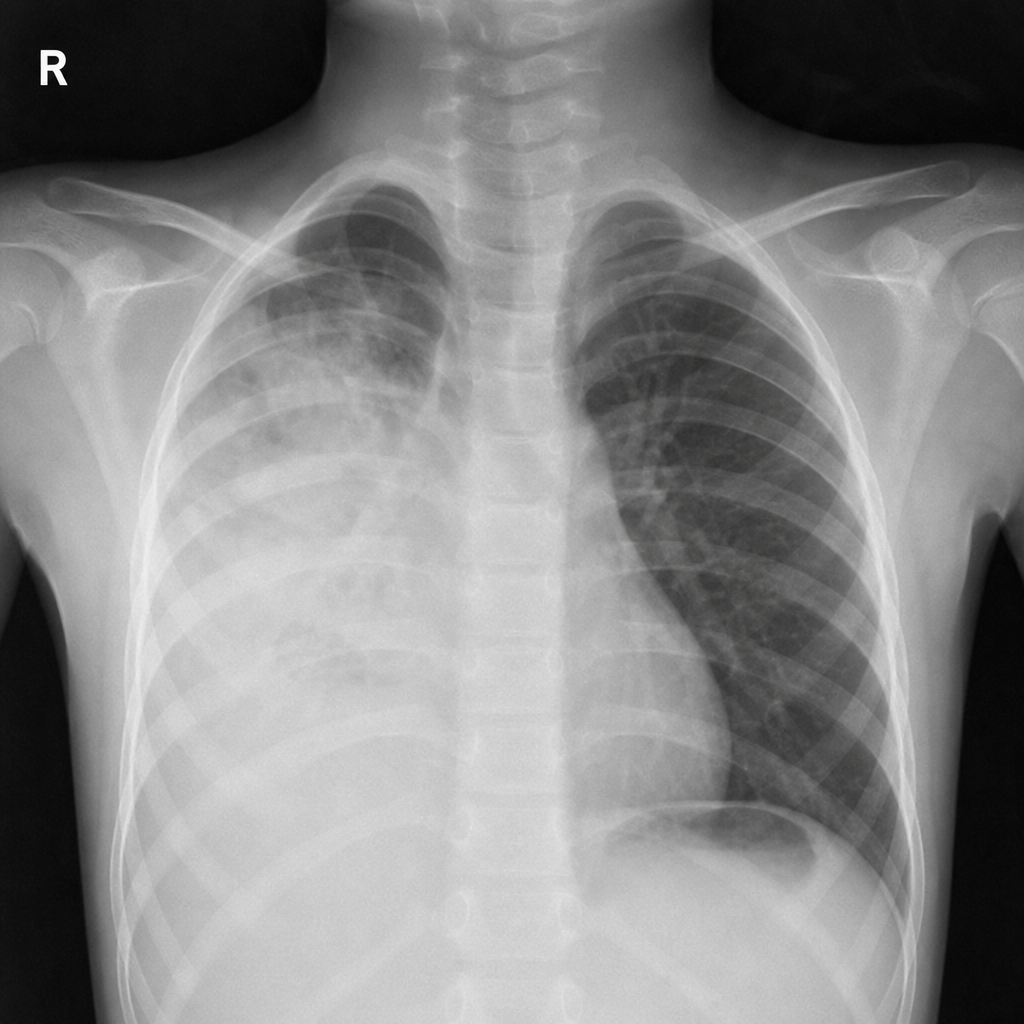
An 8-year-old child presents with a 7-month history of cough, a 1-month history of hemoptysis, and a 4-day history of fever. An X-ray shows the following findings. What is your diagnosis?
A young boy developed respiratory distress. On examination, the chest X-ray showed hyperinflation of one lung. Which of the following is the most possible diagnosis?
Practice by Chapter
Upper Respiratory Tract Infections
Practice Questions
Lower Respiratory Tract Infections
Practice Questions
Asthma Management
Practice Questions
Cystic Fibrosis
Practice Questions
Bronchiolitis
Practice Questions
Foreign Body Aspiration
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Congenital Lung Malformations
Practice Questions
Pleural Diseases
Practice Questions
Tuberculosis in Children
Practice Questions
Chronic Lung Disease in Premature Infants
Practice Questions
Pulmonary Function Testing
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app