
Respiratory Diseases — MCQs

On this page
A 3-month-old baby presents with fever and respiratory rate of 60/min. The baby is irritable but feeding well. There is no stridor, no chest indrawing, and no convulsions. What is the diagnosis?
A 6-month-old female infant is brought to the physician with a 2-day history of severe cough, wheezing, and respiratory distress. Physical examination shows rhinitis, mild cyanosis, and fever. Which of the following is the most likely etiology of this child's pulmonary infection?
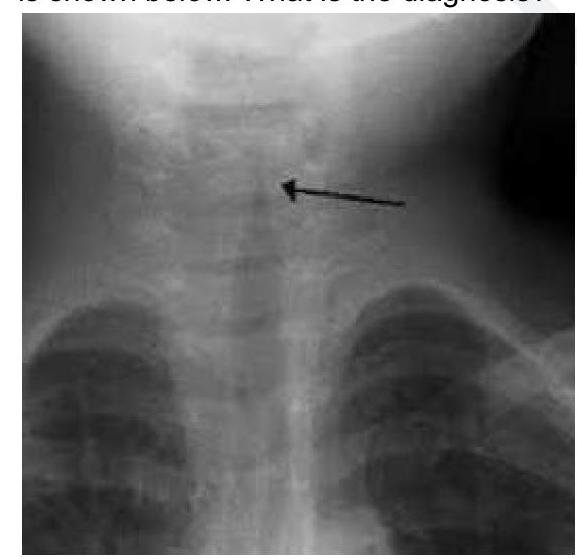
A child with acute respiratory distress showing hyperinflation of the unilateral lung in X-ray is due to –
Stridor in an infant is most commonly due to:
A 5-year old boy while having dinner suddenly becomes aphonic and is brought to the casualty with the complaint of respiratory distress. Immediate management should be:
A child is brought to the paediatric OPD with fever of 24 hours duration. History reveals 3 episodes of chest infection and passage of foul smelling stools. The most probable diagnosis is-
A month old HIV positive child following an upper respiratory infection developed sudden onset of breathlessness. The chest x-ray shows hyperinflation. The O2 saturation was greater than 90%. What is the most appropriate antiviral therapy among the given options?
A 3 month old infant presents with a 3 day history of fever, cough, and poor feeding. On examination, the baby appears ill and has a temperature of 102 F and a respiratory rate of 32. A chest x-ray film showed bilateral patchy infiltrates in the lungs. Which of the following is the most likely etiologic agent?
A 24 month child, with a weight of 11 kg, has RR of 38 / min, chest indrawing, cough and fever. Management according to IMNCI?
A 2 year child presented with low grade fever and stridor. What is the likely diagnosis?
Practice by Chapter
Upper Respiratory Tract Infections
Practice Questions
Lower Respiratory Tract Infections
Practice Questions
Asthma Management
Practice Questions
Cystic Fibrosis
Practice Questions
Bronchiolitis
Practice Questions
Foreign Body Aspiration
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Congenital Lung Malformations
Practice Questions
Pleural Diseases
Practice Questions
Tuberculosis in Children
Practice Questions
Chronic Lung Disease in Premature Infants
Practice Questions
Pulmonary Function Testing
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app