
Respiratory Diseases — MCQs

On this page
A 5-year-old child presented with recurrent respiratory infections with thickened sputum. Chest X-ray showed bronchial wall thickening. He has been suffering from steatorrhea since birth. Which of the following is the first differential diagnosis?
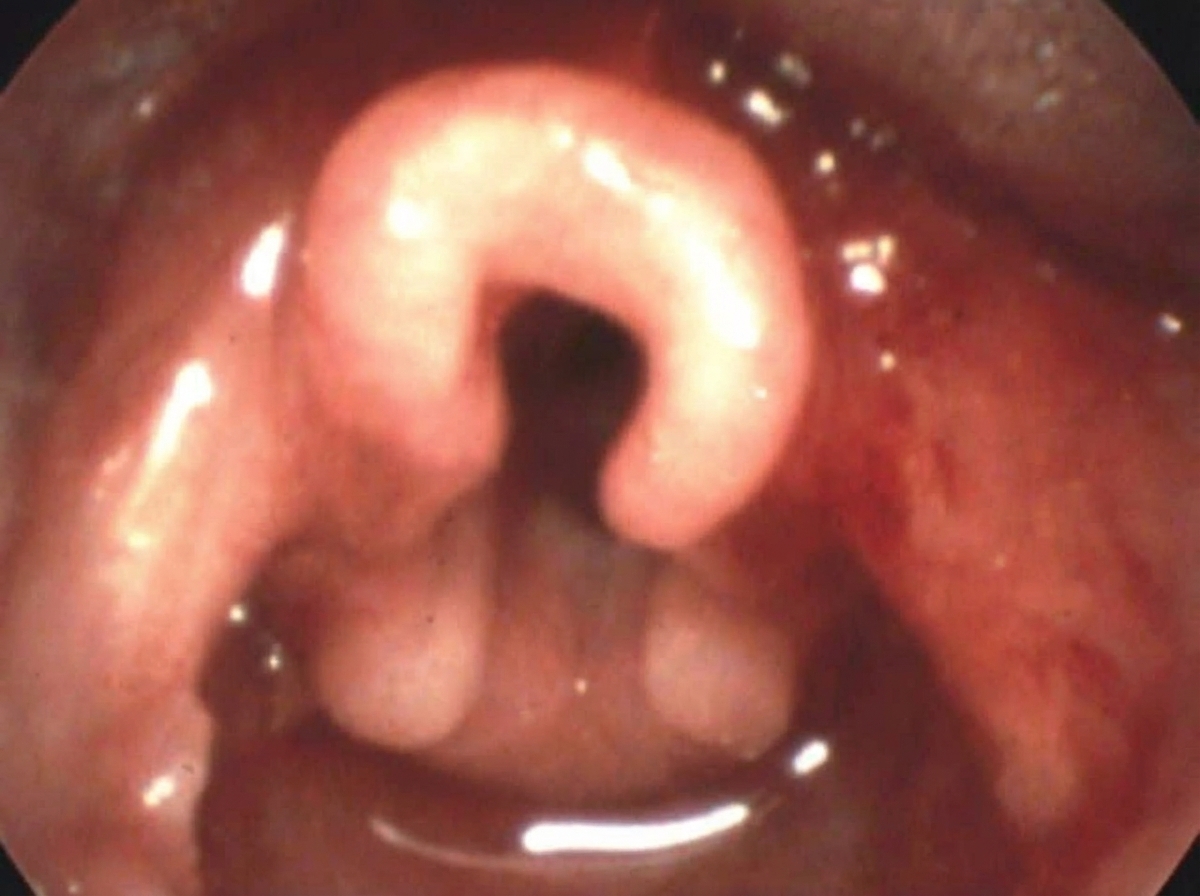
Which of the following diagnoses can cause stridor in infants? 1. Laryngomalacia 2. Congenital hemangioma 3. Subglottic stenosis 4. Recurrent respiratory papillomatosis (RRP)
Which of the following is incorrect about the clinical condition shown below?
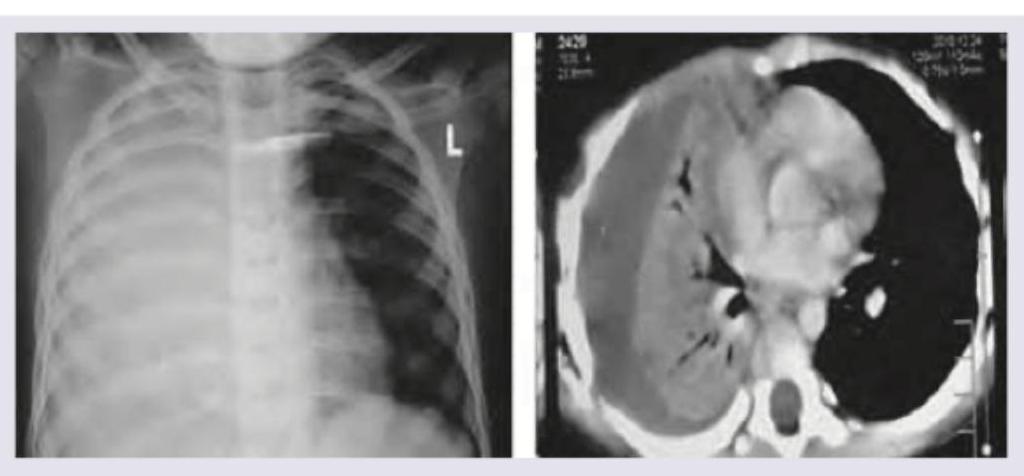
A 4-year-old child with high grade fever with chills and rigors for past 4 days and fast breathing is brought to the hospital. On examination subcostal recession and nasal flaring is noted. Since patient is already on antibiotics for past 3 days from another hospital a Chest X-ray and CT Chest was ordered. The diagnosis is:
A 4-year-old admitted in ward with pneumonia. He develops sudden onset of breathlessness. What is the next step in management?

A 10-year-old child presents with fever, chills, rigors and fast, difficult breathing. The image shows:

A 12-month-old child who was previously well presented with low grade fever and respiratory distress and on examination there is bilateral wheeze. There is a history of URI in elder sibling. What is the diagnosis?
For a sick child aged 4 years, which of the following are signs of "severe pneumonia or very severe disease", as per IMNCI (Integrated Management of Neonatal and Childhood Illness) Program? I. Fast breathing (Greater than or equal to 40 breaths per minute) II. Child vomits everything III. Stridor in a calm child IV. Chest indrawing: Select the correct answer using the code given below :
A child of 2 years having a respiratory rate of 46 per minute shall be classified by a health worker as
Which sign is most important in deciding severe pneumonia in a child?
Practice by Chapter
Upper Respiratory Tract Infections
Practice Questions
Lower Respiratory Tract Infections
Practice Questions
Asthma Management
Practice Questions
Cystic Fibrosis
Practice Questions
Bronchiolitis
Practice Questions
Foreign Body Aspiration
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Congenital Lung Malformations
Practice Questions
Pleural Diseases
Practice Questions
Tuberculosis in Children
Practice Questions
Chronic Lung Disease in Premature Infants
Practice Questions
Pulmonary Function Testing
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app