
Respiratory Diseases — MCQs

On this page
A 13-year-old known asthmatic presents with severe wheezing and a respiratory rate of 40. Her pulse rate is 120. What is the next best step in management of this patient?
A 10-year-old boy presents with a history of recurrent abdominal pain. There is a past history of bronchitis but no history of pneumonia. On examination, there has been no significant increase in weight over the past 3 years, with flattening of the growth curve. Trace digital clubbing is noted. What is the most appropriate test to be ordered at this time?
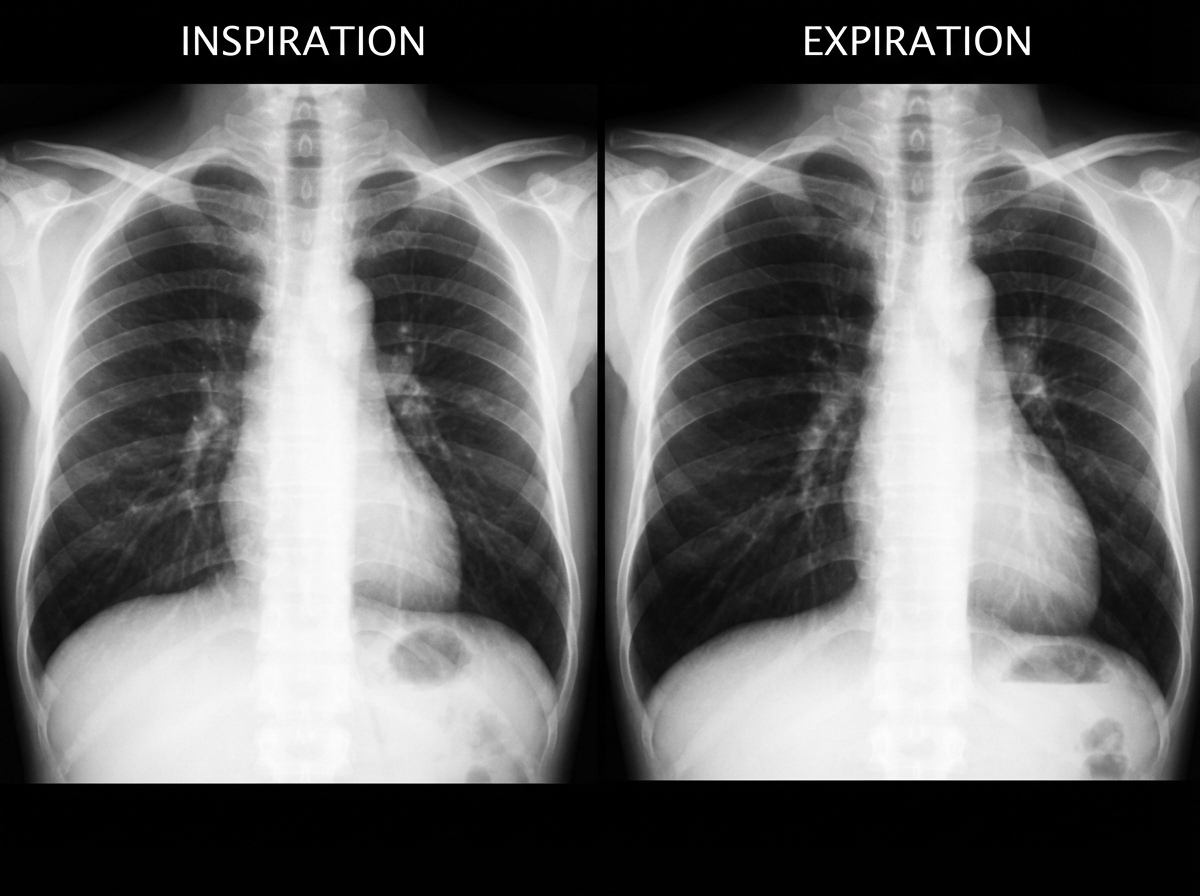
A previously healthy 2-year-old black child has developed a chronic cough during the previous 6 weeks. He has been seen in different emergency rooms on two occasions during this period and has been placed on antibiotics for pneumonia. Upon auscultation, you hear normal breath sounds on the left. On the right side, you hear decreased air movement during inspiration but no air movement upon expiration. Inspiratory and expiratory radiographs of the chest are shown. Which of the following is the most appropriate next step in making the diagnosis in this patient?
A 7.5-month-old child presents with cough and mild stridor, initially treated with oral antibiotics showing improvement. Subsequently, the child developed wheeze, productive cough, and mild fever. Radiography reveals hyperlucency, and pulmonary function tests demonstrate an obstructive pattern. What is the most probable diagnosis?
A 14-year-old boy presents with headache, fever, and cough for 2 days. Sputum is scant and non-purulent, and Gram stain reveals many white cells but no organisms. With which medication should treatment be initiated?
Which of the following is the investigation of choice for Congenital Lobar Emphysema?
A 4-year-old asthmatic child presents with inability to speak, rapid shallow breathing, and pulsus paradoxus. Arterial blood gas analysis reveals respiratory acidosis. What is the next best step in managing this patient?
Which one of the following is not a common feature of cystic fibrosis?
Which genetic mutation is most commonly associated with congenital central hypoventilation syndrome?
A 3-year-old girl presents with a high fever, anorexia, and discomfort. She is leaning forward with significant drooling. A cervical radiograph is shown. What is the most likely explanation for this finding?

Practice by Chapter
Upper Respiratory Tract Infections
Practice Questions
Lower Respiratory Tract Infections
Practice Questions
Asthma Management
Practice Questions
Cystic Fibrosis
Practice Questions
Bronchiolitis
Practice Questions
Foreign Body Aspiration
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Congenital Lung Malformations
Practice Questions
Pleural Diseases
Practice Questions
Tuberculosis in Children
Practice Questions
Chronic Lung Disease in Premature Infants
Practice Questions
Pulmonary Function Testing
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app