
Respiratory Diseases — MCQs

On this page
For a sick child aged 4 years, which of the following are signs of "severe pneumonia or very severe disease", as per IMNCI (Integrated Management of Neonatal and Childhood Illness) Program? I. Fast breathing (Greater than or equal to 40 breaths per minute) II. Child vomits everything III. Stridor in a calm child IV. Chest indrawing: Select the correct answer using the code given below :
A 15-month-old child presents with fever and cough since the last two days, the respiratory rate is 55/min and there is no drawing of the chest. According to the National Programme for Acute Respiratory Infections, the line of management should be
A child of 2 years having a respiratory rate of 46 per minute shall be classified by a health worker as
Which sign is most important in deciding severe pneumonia in a child?
The recommended dose of cotrimoxazole for treatment of pneumonia in a child weighing 16 kg is
A 3-month-old baby presents with fever and respiratory rate of 60/min. The baby is irritable but feeding well. There is no stridor, no chest indrawing, and no convulsions. What is the diagnosis?
A 6-month-old female infant is brought to the physician with a 2-day history of severe cough, wheezing, and respiratory distress. Physical examination shows rhinitis, mild cyanosis, and fever. Which of the following is the most likely etiology of this child's pulmonary infection?
A child with acute respiratory distress showing hyperinflation of the unilateral lung in X-ray is due to –
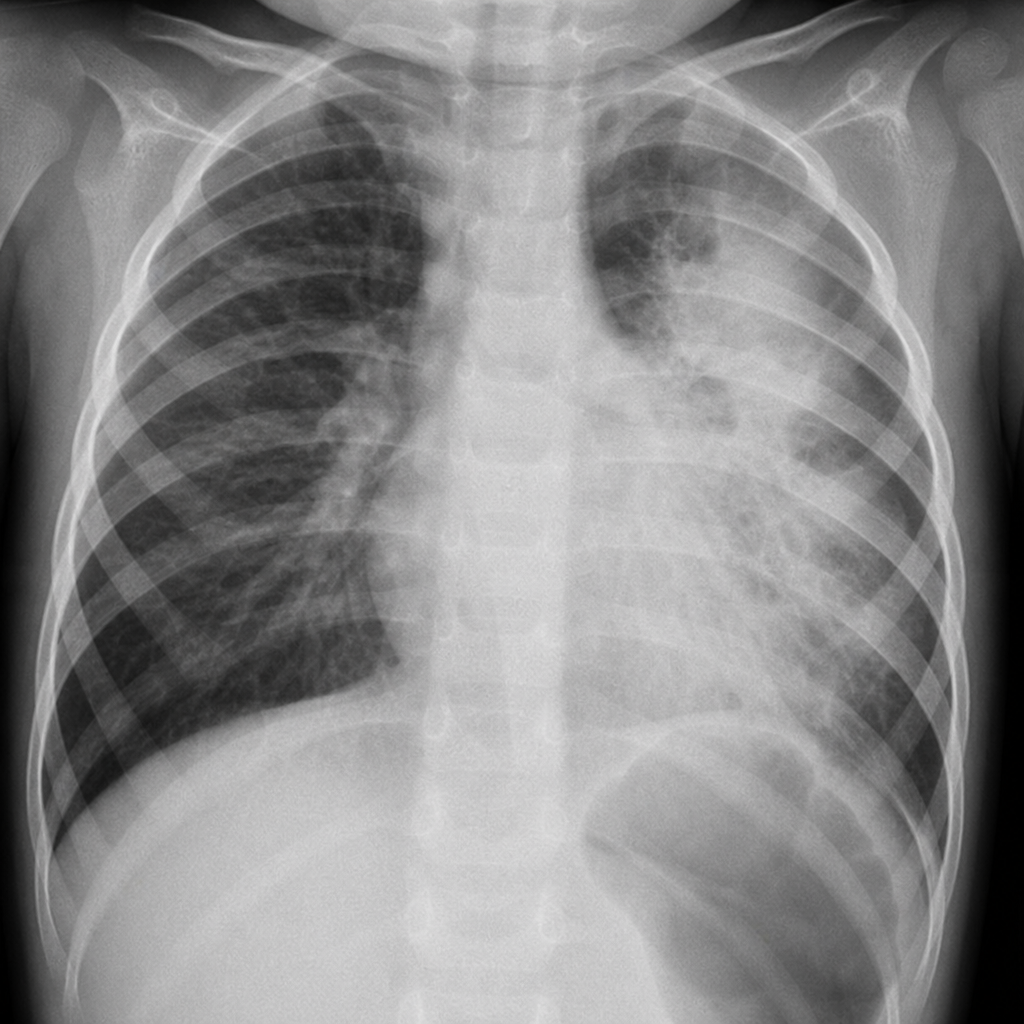
A 3 year old non-vaccinated child presented with fever and fast breathing. His mother reported that he has recently developed measles rash. CXR shown below is indicative of which infection?
The commonest cause of Bacterial Pneumonia in children is -
Practice by Chapter
Upper Respiratory Tract Infections
Practice Questions
Lower Respiratory Tract Infections
Practice Questions
Asthma Management
Practice Questions
Cystic Fibrosis
Practice Questions
Bronchiolitis
Practice Questions
Foreign Body Aspiration
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Congenital Lung Malformations
Practice Questions
Pleural Diseases
Practice Questions
Tuberculosis in Children
Practice Questions
Chronic Lung Disease in Premature Infants
Practice Questions
Pulmonary Function Testing
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app