
Respiratory Diseases — MCQs

On this page
Aerosolized ribavirin is used in the treatment of bronchiolitis with which causative organism?
Which of the following is seen in cystic fibrosis?
A child presents with recurrent sinusitis and repeated lung infections. Genetic testing shows a mutation in the CFTR gene. Which test is considered the gold standard to confirm the diagnosis?
A 4-month-old infant is brought to the emergency department with a respiratory rate of 66 breaths per minute, along with chest indrawing and nasal flaring. There are no other significant findings. What is the most likely diagnosis?
A 3-month-old child has a respiratory rate of 56/min with no chest indrawing and no danger signs. As per IMNCI what is the most appropriate diagnosis?
A 5-year-old child presented with recurrent respiratory infections with thickened sputum. Chest X-ray showed bronchial wall thickening. He has been suffering from steatorrhea since birth. Which of the following is the first differential diagnosis?
A 4-year-old admitted in ward with pneumonia. He develops sudden onset of breathlessness with rapidly deteriorating respiratory status and hemodynamic compromise (hypotension, tachycardia). What is the next step in management?

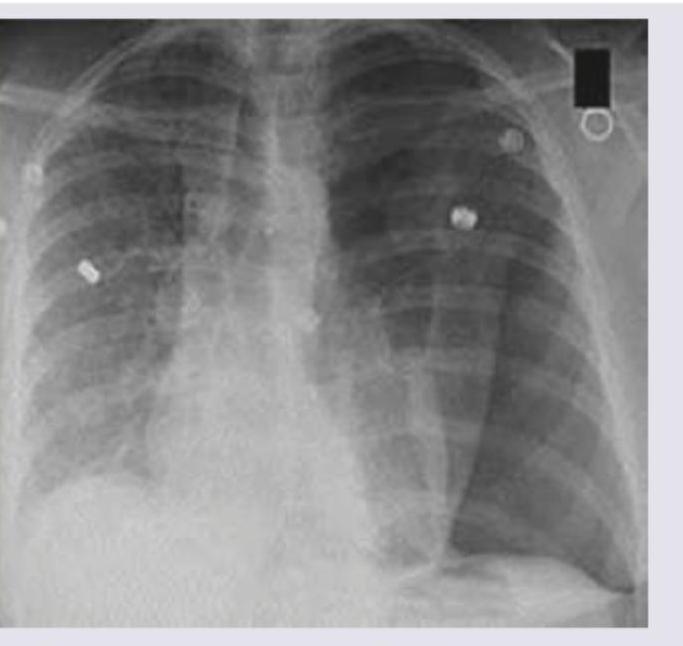
A 10-year-old child presents with fever, chills, rigors and fast, difficult breathing. The image shows:

A 12-month-old child who was previously well presented with low grade fever and respiratory distress and on examination there is bilateral wheeze. There is a history of URI in elder sibling. What is the diagnosis?
A 1-year-old child with severe acute malnutrition develops pneumonia which is not responding to treatment. Chest X-ray picture is given. What is the likely etiology?
Practice by Chapter
Upper Respiratory Tract Infections
Practice Questions
Lower Respiratory Tract Infections
Practice Questions
Asthma Management
Practice Questions
Cystic Fibrosis
Practice Questions
Bronchiolitis
Practice Questions
Foreign Body Aspiration
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Congenital Lung Malformations
Practice Questions
Pleural Diseases
Practice Questions
Tuberculosis in Children
Practice Questions
Chronic Lung Disease in Premature Infants
Practice Questions
Pulmonary Function Testing
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app