
Respiratory Diseases — MCQs

On this page
Crackles are frequently heard in which of the following conditions?
A 6-week-old baby presents with cough and cold for the past 3 days. The respiratory rate is 48/min. On examination, the patient is febrile with wheezing but no chest indrawing. Which of the following statements is not true?
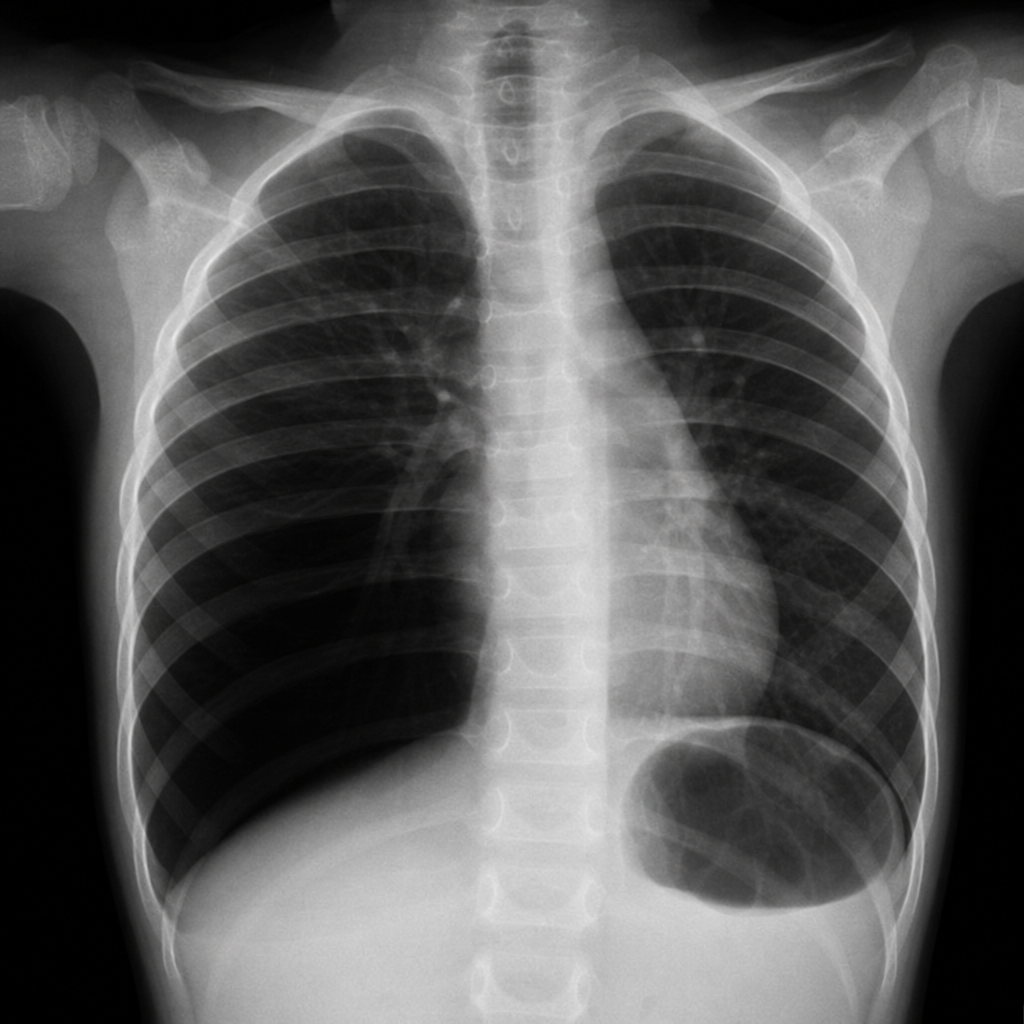
A 4-year-old child developed sudden bouts of cough and respiratory distress after eating peanuts. Chest X-ray findings are provided. What is the diagnosis?
An 18-month-old child weighing 11.5 kg presents to the primary health center with fever and respiratory difficulty. On examination, the child is lethargic, with a respiratory rate of 46 bpm and no chest retractions. What is the most appropriate management of this child?
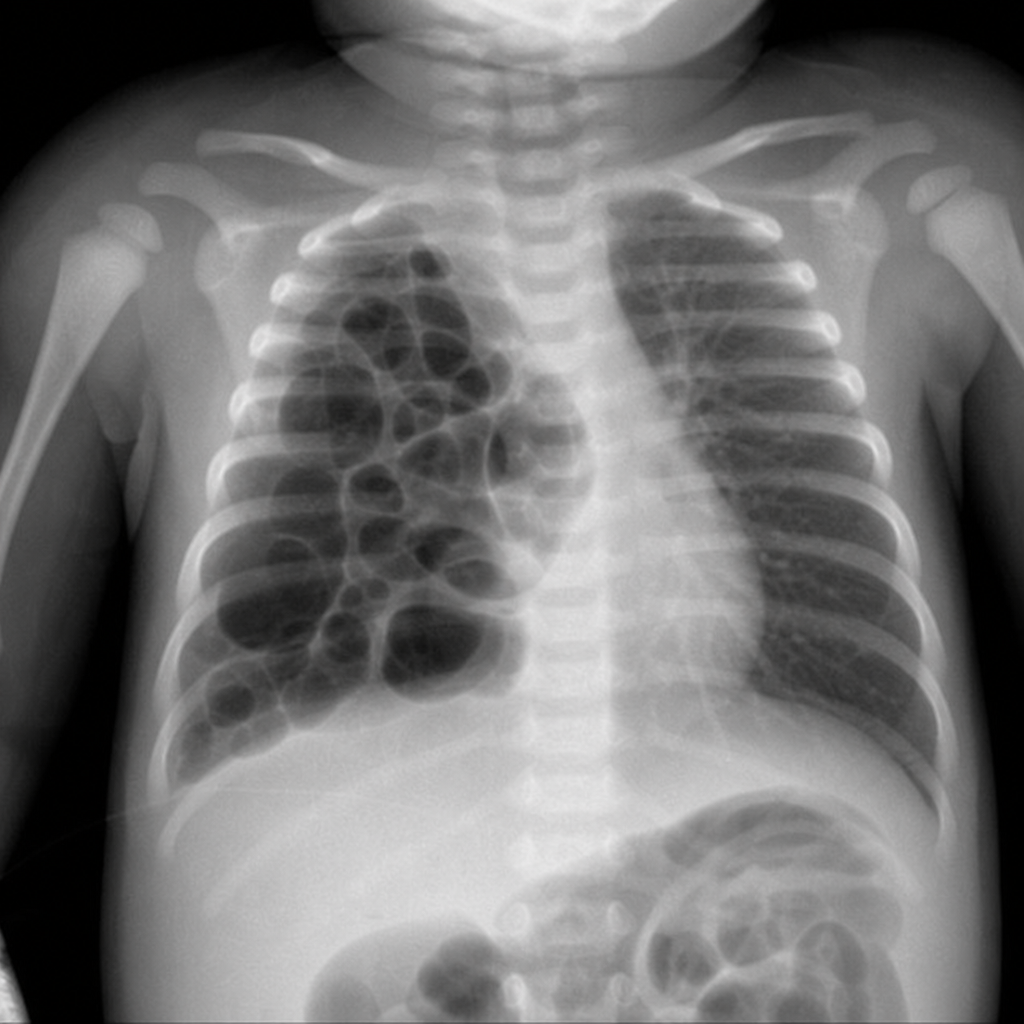
A neonate is suffering from respiratory distress. A chest X-ray shows multiple air-filled spaces. What is the most likely diagnosis?
A healthy 10-year-old boy presents with fever, cough, and lower respiratory symptoms of 5 days duration. Auscultatory findings are consistent with pneumonia. What is the first-line drug for this condition?
A child presents with stridor, barking cough, and difficulty in breathing for 2-3 days. The child has a fever and an elevated leukocyte count. Which of the following statements about this condition is FALSE?
What is the most likely cause of bronchiolitis in a 6-month-old infant?
A 3-year-old child presents to a primary health center with fever, chest indrawing, and a respiratory rate of 38 per minute. What is the next step in management?
Which of the following is NOT a feature of Cystic fibrosis?
Practice by Chapter
Upper Respiratory Tract Infections
Practice Questions
Lower Respiratory Tract Infections
Practice Questions
Asthma Management
Practice Questions
Cystic Fibrosis
Practice Questions
Bronchiolitis
Practice Questions
Foreign Body Aspiration
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Congenital Lung Malformations
Practice Questions
Pleural Diseases
Practice Questions
Tuberculosis in Children
Practice Questions
Chronic Lung Disease in Premature Infants
Practice Questions
Pulmonary Function Testing
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app