
Respiratory Diseases — MCQs

On this page
A 4-year-old child with bronchial asthma presents with 3 or more episodes of wheezing during the daytime in a week and 2 wheezing episodes during the night in a month. How will you grade this asthma?
A 3-month-old child presents with biphasic stridor and barking cough. All of the following are true regarding this condition EXCEPT:
In a 3-year-old child, what respiratory rate is classified as Pneumonia?
A seven-year-old child presents with recurrent chest infections and exocrine pancreatic insufficiency, raising suspicion for cystic fibrosis. Sweat chloride levels have been measured between 40-60 mmol/l on two separate occasions. Which of the following tests should be performed next to support the diagnosis of cystic fibrosis?
"Steeple sign" on X-ray in children is most likely indicative of which condition?
What is true regarding bronchiolitis obliterans without cyanosis?
A 2-year-old boy presented with cough, fever, and difficulty in breathing. His respiratory rate is 50/min. There is no chest indrawing. Auscultation of the chest reveals bilateral crepitations. What is the most probable diagnosis?
All of the following are useful for treating acute bronchial asthma in children except?
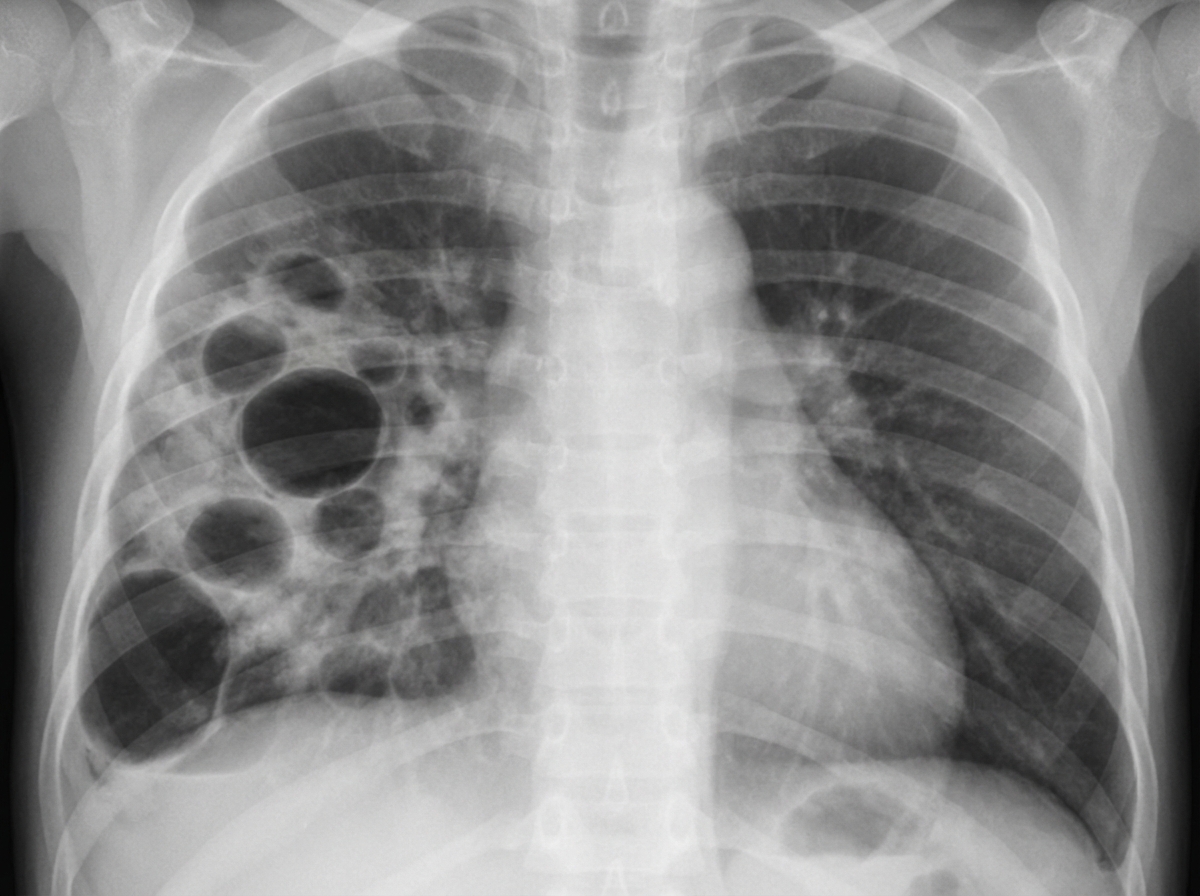
An infant presented to OPD with features of respiratory distress. The X-ray is shown below. The most probable organism is?
What is the drug of choice for the prophylaxis of Bronchiolitis in a child with heart disease?
Practice by Chapter
Upper Respiratory Tract Infections
Practice Questions
Lower Respiratory Tract Infections
Practice Questions
Asthma Management
Practice Questions
Cystic Fibrosis
Practice Questions
Bronchiolitis
Practice Questions
Foreign Body Aspiration
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Congenital Lung Malformations
Practice Questions
Pleural Diseases
Practice Questions
Tuberculosis in Children
Practice Questions
Chronic Lung Disease in Premature Infants
Practice Questions
Pulmonary Function Testing
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app