
Pediatric Surgery Basics — MCQs

On this page
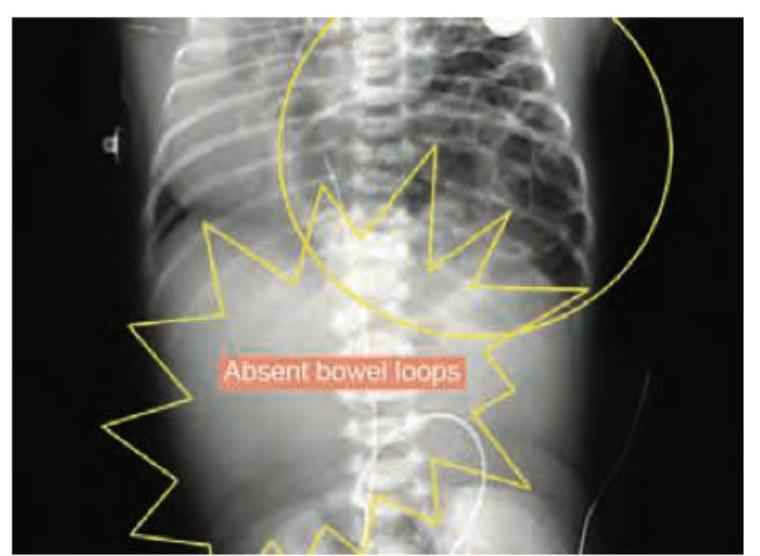
A newborn presents with respiratory distress shortly after birth. The chest X-ray shows bowel loops in the thoracic cavity and absence of bowel loops in the abdominal area. There is associated hypoplasia of the ipsilateral lung. What is the most likely diagnosis?
A child with cleft palate is shown. All are seen in this child except:
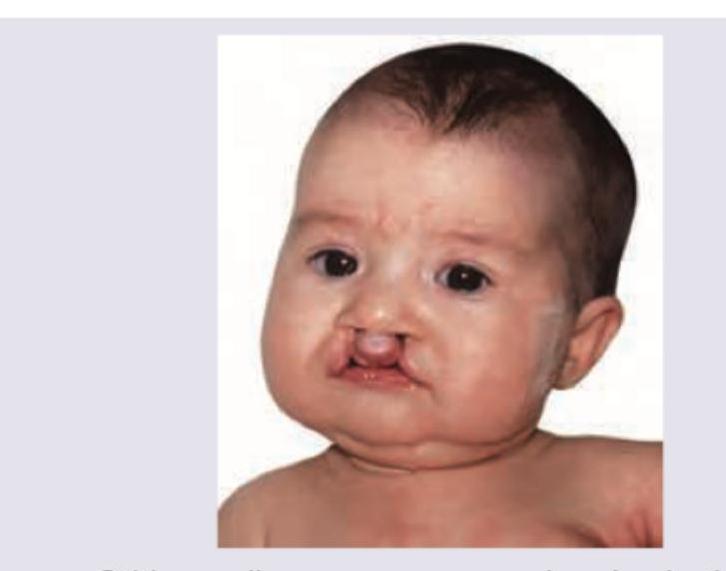
A four-month-old baby has cleft lip and palate. How would you manage the baby?
Consider the following conditions: 1. Otitis media 2. Speech problems 3. Dentition abnormalities Which of the above is/are associated with cleft palate?
A five-year-old child presents with ballooning of prepuce after micturition. Examination reveals preputial adhesions. Which of the following is the best treatment?
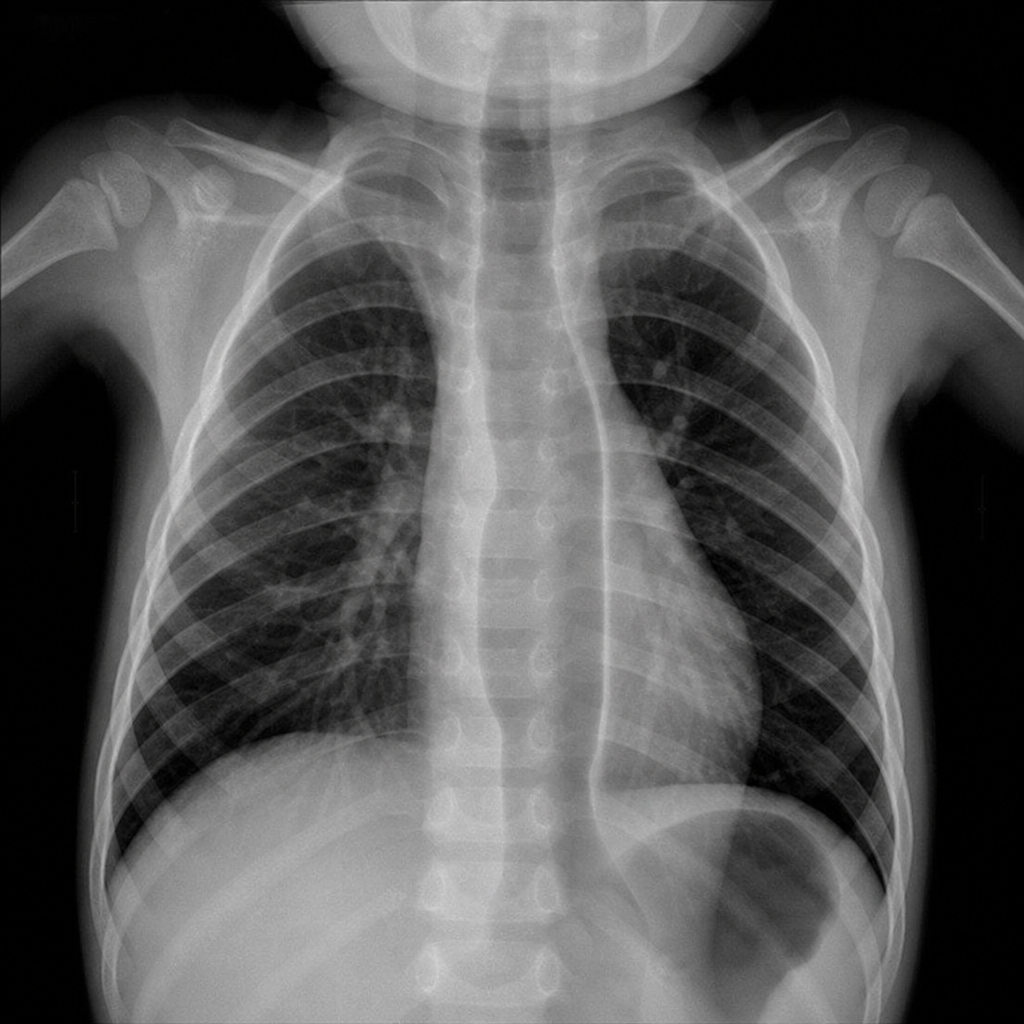
A 2-year-old boy presented to the ER with stridor, shortness of breath, and difficulty in swallowing. The patient also has a history of recurrent chest infections in the past, for which the child was frequently hospitalized. Upper GI endoscopy was normal. Lab findings revealed normal studies. Barium swallow demonstrating a posterior esophageal indentation caused by an aberrant right subclavian artery. What is the most likely diagnosis?
Esophageal atresia may occur as a part of VACTERL group of anomalies. What does 'TE' stand for?
A child presents with painful limp and restricted hip rotation. ESR and CRP are elevated. Initial plain radiograph is normal. What is the next best imaging study?
True about congenital diaphragmatic hernia (CDH) except:
A newborn presents with bilious vomiting and abdominal distension. An X-ray shows a 'double bubble' sign. What is the most likely diagnosis?
Practice by Chapter
Surgical Conditions of the Newborn
Practice Questions
Congenital Diaphragmatic Hernia
Practice Questions
Esophageal Atresia and Tracheoesophageal Fistula
Practice Questions
Intestinal Atresia and Stenosis
Practice Questions
Malrotation and Volvulus
Practice Questions
Hirschsprung's Disease
Practice Questions
Anorectal Malformations
Practice Questions
Biliary Atresia
Practice Questions
Abdominal Wall Defects
Practice Questions
Inguinal Hernia and Hydrocele
Practice Questions
Intussusception
Practice Questions
Appendicitis in Children
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app