
Pediatric Surgery Basics — MCQs

On this page
What is the most common type of congenital atresia?
Which electrolyte should be replenished in hypertrophic pyloric stenosis?
What is true about Bochdalek hernia?
A 9-month-old girl presents with perianal bleeding, vomiting, a right lumbar mass, and masked liver dullness. She is in a shock-like condition. Management should include all of the following EXCEPT?
Which of the following is true for Bochdalek hernia?
The image shows:

What is the malformation shown in the image?
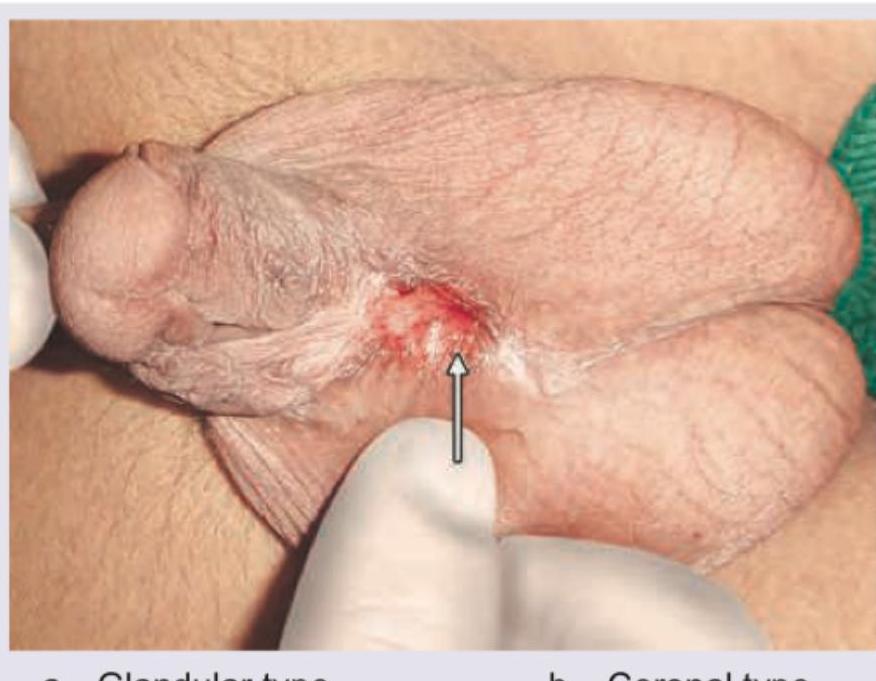
The image shows:

A newborn presents with respiratory distress shortly after birth. The chest X-ray shows bowel loops in the thoracic cavity and absence of bowel loops in the abdominal area. There is associated hypoplasia of the ipsilateral lung. What is the most likely diagnosis?
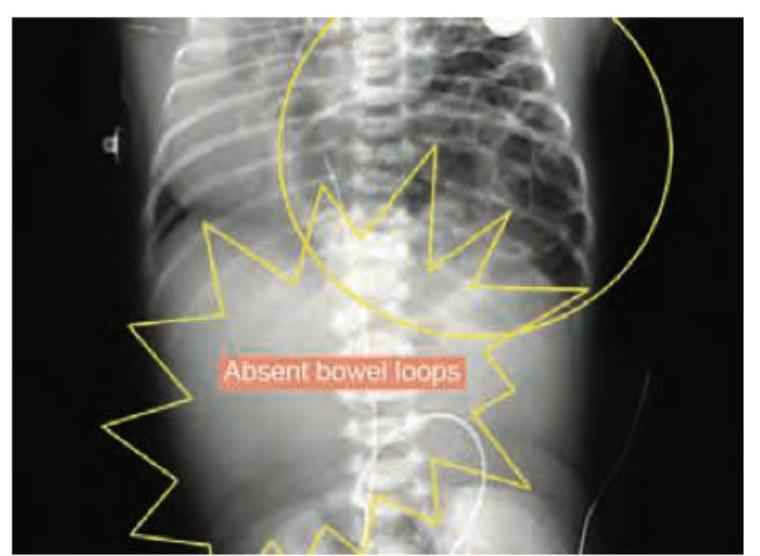
All are true about the condition shown in the figure except:

Practice by Chapter
Surgical Conditions of the Newborn
Practice Questions
Congenital Diaphragmatic Hernia
Practice Questions
Esophageal Atresia and Tracheoesophageal Fistula
Practice Questions
Intestinal Atresia and Stenosis
Practice Questions
Malrotation and Volvulus
Practice Questions
Hirschsprung's Disease
Practice Questions
Anorectal Malformations
Practice Questions
Biliary Atresia
Practice Questions
Abdominal Wall Defects
Practice Questions
Inguinal Hernia and Hydrocele
Practice Questions
Intussusception
Practice Questions
Appendicitis in Children
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app