
Pediatric Surgery Basics — MCQs

On this page
What is the diagnosis of a child presenting with a pulsatile swelling on the medial side of the nose?
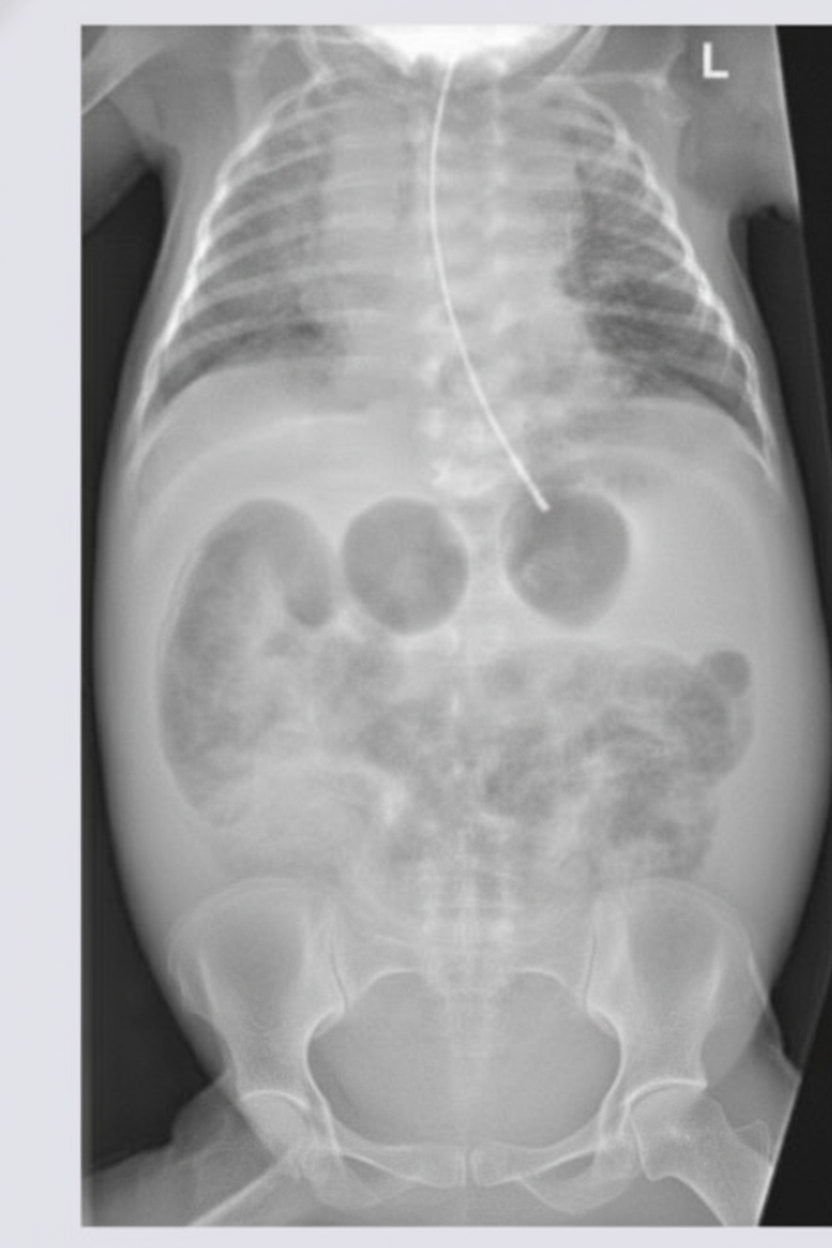
A newborn infant presents with a history of multiple episodes of bilious projectile vomiting. An X-ray of the abdomen was performed. What is the most likely diagnosis?
What is the most likely diagnosis?

Which of the following is NOT true about congenital hypertrophic pyloric stenosis (CHPS)?
What is the most common type of diaphragmatic hernia in children?
What is the commonest cause of intestinal obstruction in a newborn?
What is the most common type of dental caries seen in a primary first molar?
A child underwent splenectomy for splenic injury and blood loss following trauma. What is the recommended further management, considering all EXCEPT which of the following?
True regarding cystic hygroma is:
The covering over an omphalocele is?
Practice by Chapter
Surgical Conditions of the Newborn
Practice Questions
Congenital Diaphragmatic Hernia
Practice Questions
Esophageal Atresia and Tracheoesophageal Fistula
Practice Questions
Intestinal Atresia and Stenosis
Practice Questions
Malrotation and Volvulus
Practice Questions
Hirschsprung's Disease
Practice Questions
Anorectal Malformations
Practice Questions
Biliary Atresia
Practice Questions
Abdominal Wall Defects
Practice Questions
Inguinal Hernia and Hydrocele
Practice Questions
Intussusception
Practice Questions
Appendicitis in Children
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app