
Pediatric Nutrition — MCQs

On this page
In infants and toddlers, craniotabes is a sign related to the deficiency of
Among the following, the best indicator for acute malnutrition in the under-fives is
Which of the following criteria are used for detecting a child with severe acute malnutrition according to WHO guidelines? 1. Bilateral pitting oedema 2. Weight for height Z-score less than minus three SD 3. Mid upper arm circumference of less than 11.5 cm (115 mm) Select the correct answer using the code given below:
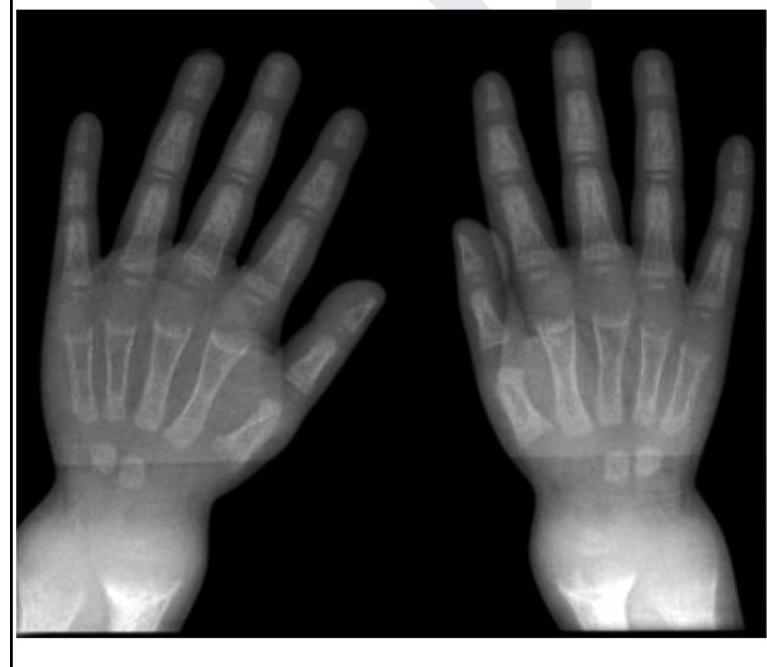
A child presents with poor growth and swelling at joints. A radiograph of his wrist is given below. Lab investigations reveal serum ALP levels of >1500. What is the possible diagnosis?
Dose of vitamin A for an 18 month old baby, with keratomalacia, weighing 10 kg is?
Which is the most specific clinical feature for diagnosis of Kwashiorkor?
For severe acute malnutrition in children (6-59 months), MAC will be less than
In marasmus, which of the following is characteristically seen?
A breast fed child presents with hypernatremia (Serum sodium > 170m Eq/L). His urine sodium is 70 mEq/L. Which of the following is the most likely cause –
Craniotabes is seen in
Practice by Chapter
Breastfeeding
Practice Questions
Infant Formula Feeding
Practice Questions
Complementary Feeding
Practice Questions
Nutritional Requirements by Age
Practice Questions
Malnutrition and Failure to Thrive
Practice Questions
Obesity in Children
Practice Questions
Vitamin Deficiencies
Practice Questions
Mineral Deficiencies
Practice Questions
Food Allergies and Intolerances
Practice Questions
Nutritional Management of Chronic Diseases
Practice Questions
Eating Disorders
Practice Questions
Parenteral and Enteral Nutrition
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app