
Pediatric Nutrition — MCQs

On this page
A 4-year-old unvaccinated child presents with fever, rash, and Bitot spots. What is the appropriate line of management?
A 4-year-old child with mid-arm circumference of 105mm, upon providing therapeutic food, eagerly completed all of it. This patient is considered under?
Chronic malnutrition is best measured by?
For how long is exclusive breastfeeding recommended?
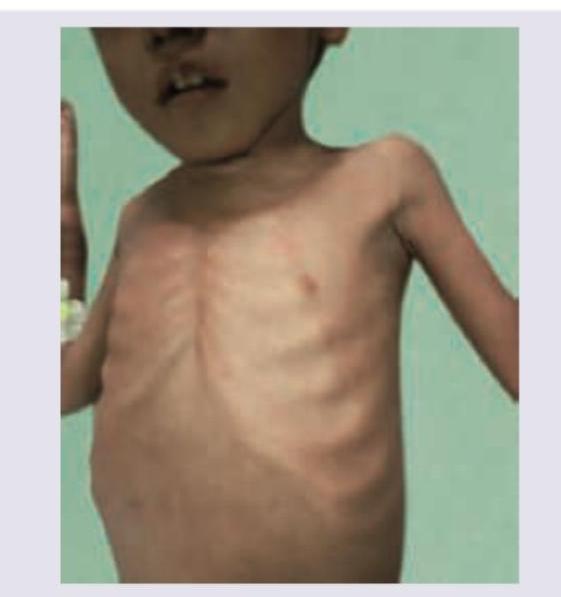
A child presents with the findings shown in the image below. What is the true statement regarding this condition?
Which of the following is an absolute contraindication for breastfeeding?
Which of the following is not true regarding Marasmus in a child?
Which of the following is/are incorrect regarding breastfeeding technique? 1. Infant's chin should be touching the breast 2. Infant's lower lip should be inverted during latching to the breast 3. A greater part of areola above the breast should be covered than below 4. Infant's cheeks should appear full during effective sucking.
A child is brought from a rural village with complaints of dry skin as shown in the image. Which vitamin deficiency is anticipated?

The following image shows the presence of?
Practice by Chapter
Breastfeeding
Practice Questions
Infant Formula Feeding
Practice Questions
Complementary Feeding
Practice Questions
Nutritional Requirements by Age
Practice Questions
Malnutrition and Failure to Thrive
Practice Questions
Obesity in Children
Practice Questions
Vitamin Deficiencies
Practice Questions
Mineral Deficiencies
Practice Questions
Food Allergies and Intolerances
Practice Questions
Nutritional Management of Chronic Diseases
Practice Questions
Eating Disorders
Practice Questions
Parenteral and Enteral Nutrition
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app