
Pediatric Nutrition — MCQs

On this page
An 8-month-old infant is being treated with vitamin A supplementation over 2 consecutive days for Vitamin A deficiency. What is the recommended dose to be given each day?
A primigravida delivers a healthy baby via normal delivery. After how many hours should she initiate breastfeeding?
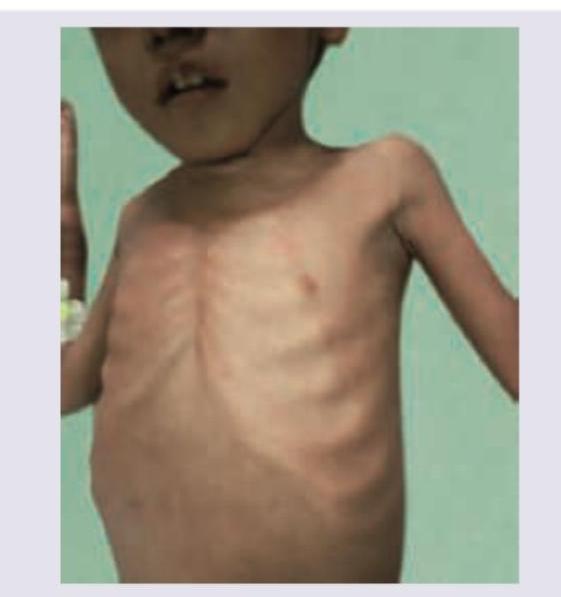
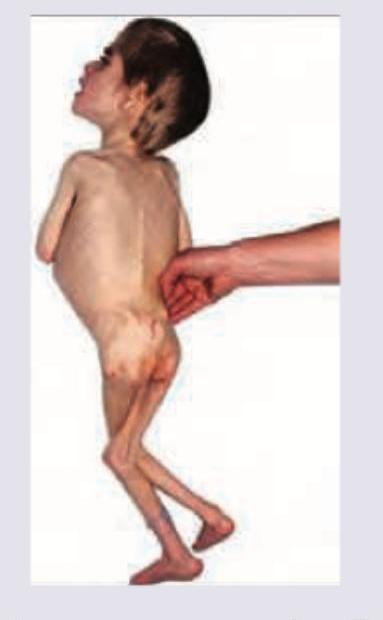
Which of the following is not true regarding Marasmus in a child?
Which of the following is/are incorrect regarding breastfeeding technique? 1. Infant's chin should be touching the breast 2. Infant's lower lip should be inverted during latching to the breast 3. A greater part of areola above the breast should be covered than below 4. Infant's cheeks should appear full during effective sucking.
A child is brought from a rural village with complaints of dry skin and night blindness as shown in the image. Which vitamin deficiency is anticipated?

The following image shows the presence of?
Select the false statement regarding the disease depicted in the picture?

All are true about the child shown in the image except:
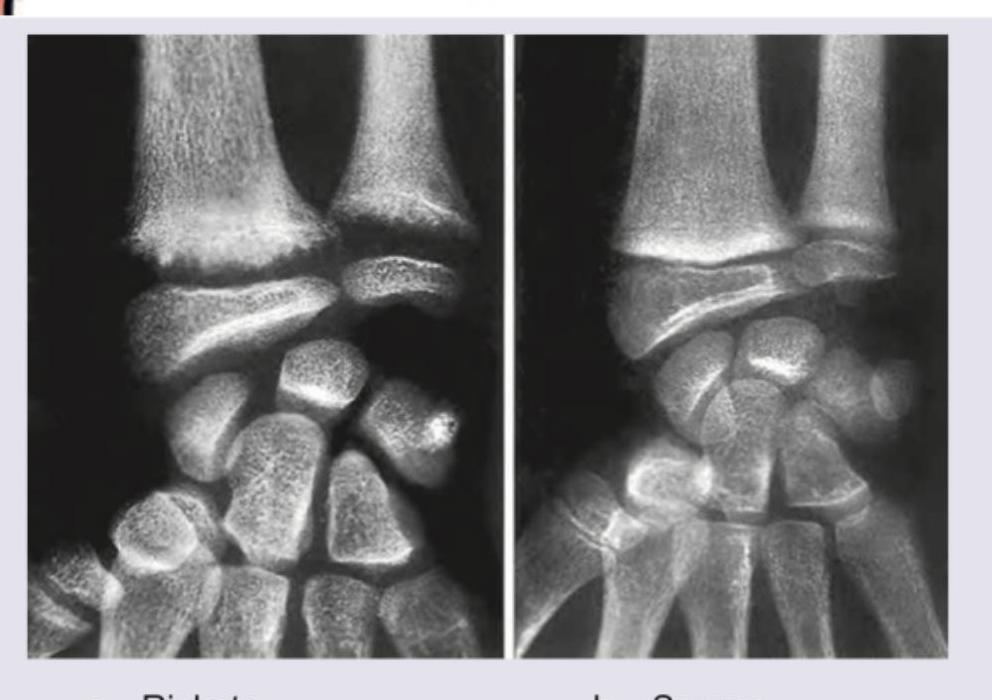
A 2-year-old child presents with delayed motor milestones and bowing of legs. X-ray of the wrist is shown. What is the most likely diagnosis?
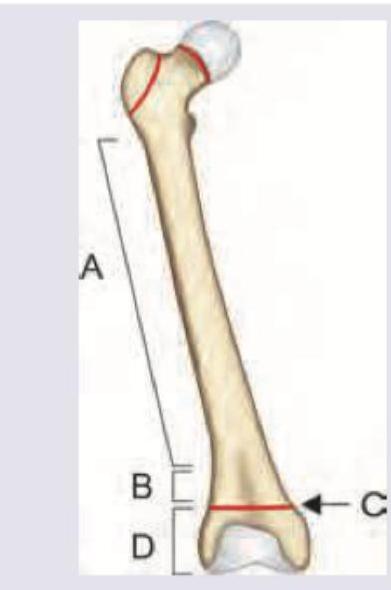
In a child with rickets, which part of the bone is the site of defective mineralization at the growth plate?
Practice by Chapter
Breastfeeding
Practice Questions
Infant Formula Feeding
Practice Questions
Complementary Feeding
Practice Questions
Nutritional Requirements by Age
Practice Questions
Malnutrition and Failure to Thrive
Practice Questions
Obesity in Children
Practice Questions
Vitamin Deficiencies
Practice Questions
Mineral Deficiencies
Practice Questions
Food Allergies and Intolerances
Practice Questions
Nutritional Management of Chronic Diseases
Practice Questions
Eating Disorders
Practice Questions
Parenteral and Enteral Nutrition
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app