
Pediatric Nutrition — MCQs

On this page
Which of the following is NOT a criterion for severe acute malnutrition in a 6-month-old child?
All of the following are true about cow's milk EXCEPT?
What are the approximate calories in human milk per 100 mL?
The length of the feeding tube to be inserted for transpyloric feeding is measured from which anatomical landmark to the umbilicus?
Compared with cow's milk, mother's milk has more-
What is the initial protein requirement of a child with Kwashiorkor in g/kg/day?
All of the following are absolute contraindications to breastfeeding except?
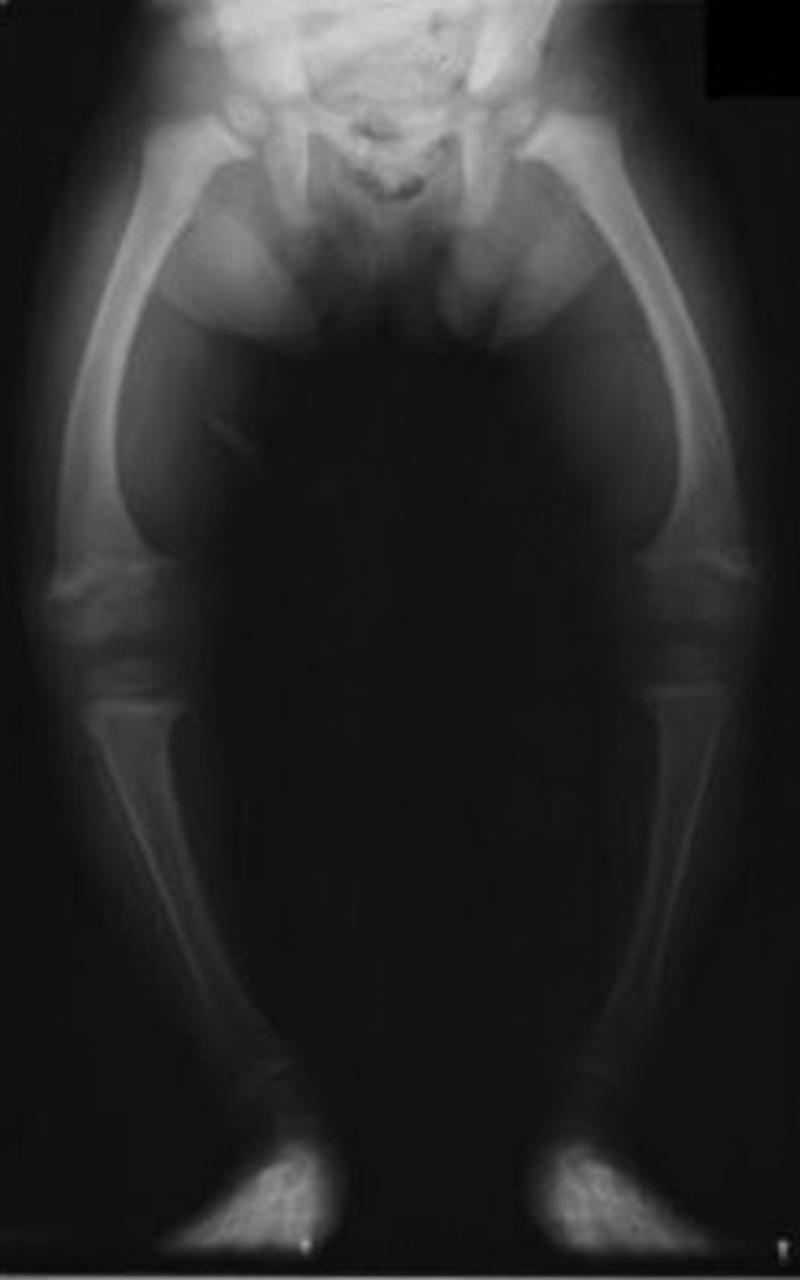
The most likely diagnosis in this child is:
All of the following are characteristic features of Kwashiorkar, except?
All of the following are true about rickets except?
Practice by Chapter
Breastfeeding
Practice Questions
Infant Formula Feeding
Practice Questions
Complementary Feeding
Practice Questions
Nutritional Requirements by Age
Practice Questions
Malnutrition and Failure to Thrive
Practice Questions
Obesity in Children
Practice Questions
Vitamin Deficiencies
Practice Questions
Mineral Deficiencies
Practice Questions
Food Allergies and Intolerances
Practice Questions
Nutritional Management of Chronic Diseases
Practice Questions
Eating Disorders
Practice Questions
Parenteral and Enteral Nutrition
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app