
Oncology — MCQs

On this page
A 5-year-old child presents with a history of fever off and on for the past 2 weeks, petechial spots all over the body, and increasing pallor for the past 1 month. Examination reveals splenomegaly of 2 cm below the costal margin. What is the most likely diagnosis?
What is the most common tumor of the face in children?
Which of the following is NOT a characteristic feature of neuroblastoma in children?
A child presents with hemihypertrophy (left arm and leg appear larger than the right) and aniridia. There is no family history of aniridia or hemihypertrophy. Which of the following is the most likely associated major abnormality in this patient?
A 1.5-year-old female presents with excessive head enlargement, feeding intolerance, and severe malnutrition. MRI suggests a medulloblastoma causing obstructive hydrocephalus. Which of the following represents an irrational management approach for this patient?
All are true about the presentation of Wilms tumor, except?
Which of the following is NOT a favorable prognostic marker in pediatric acute lymphoblastic leukemia (ALL)?
A 9-year-old boy presents with fever, feeling unwell, and easy bruising on his legs. On examination, he is pale, with a blood pressure of 100/60 mm Hg, pulse of 100/min, and a temperature of 37.8°C. His lungs are clear, his abdomen is soft with a palpable spleen, and there are petechiae and bruises on his legs. His CBC reveals a hemoglobin of 8.5 g/dL, WBC of 17,000/mL, and platelets of 30,000/mL. A blood film reveals neutropenia and leukemic lymphoblasts. What is the most appropriate initial diagnostic test to confirm the diagnosis?
Which of the following is a definite marker for hepatoblastoma?
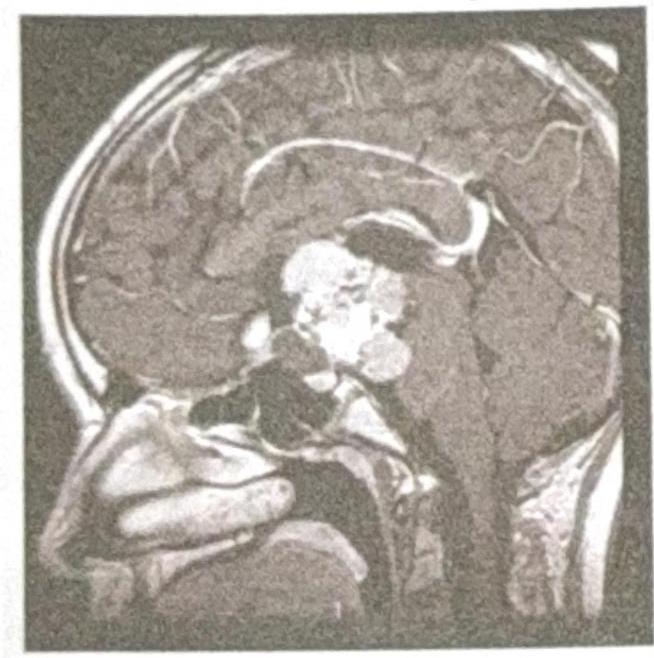
A 9-year-old female child presents with a history of headache and visual disturbances. What is the most likely diagnosis?
Practice by Chapter
Leukemias
Practice Questions
Lymphomas
Practice Questions
CNS Tumors
Practice Questions
Neuroblastoma
Practice Questions
Wilms Tumor
Practice Questions
Rhabdomyosarcoma
Practice Questions
Bone Tumors
Practice Questions
Retinoblastoma
Practice Questions
Histiocytosis Syndromes
Practice Questions
Principles of Pediatric Chemotherapy
Practice Questions
Hematopoietic Stem Cell Transplantation
Practice Questions
Late Effects of Cancer Treatment
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app