
Oncology — MCQs

On this page
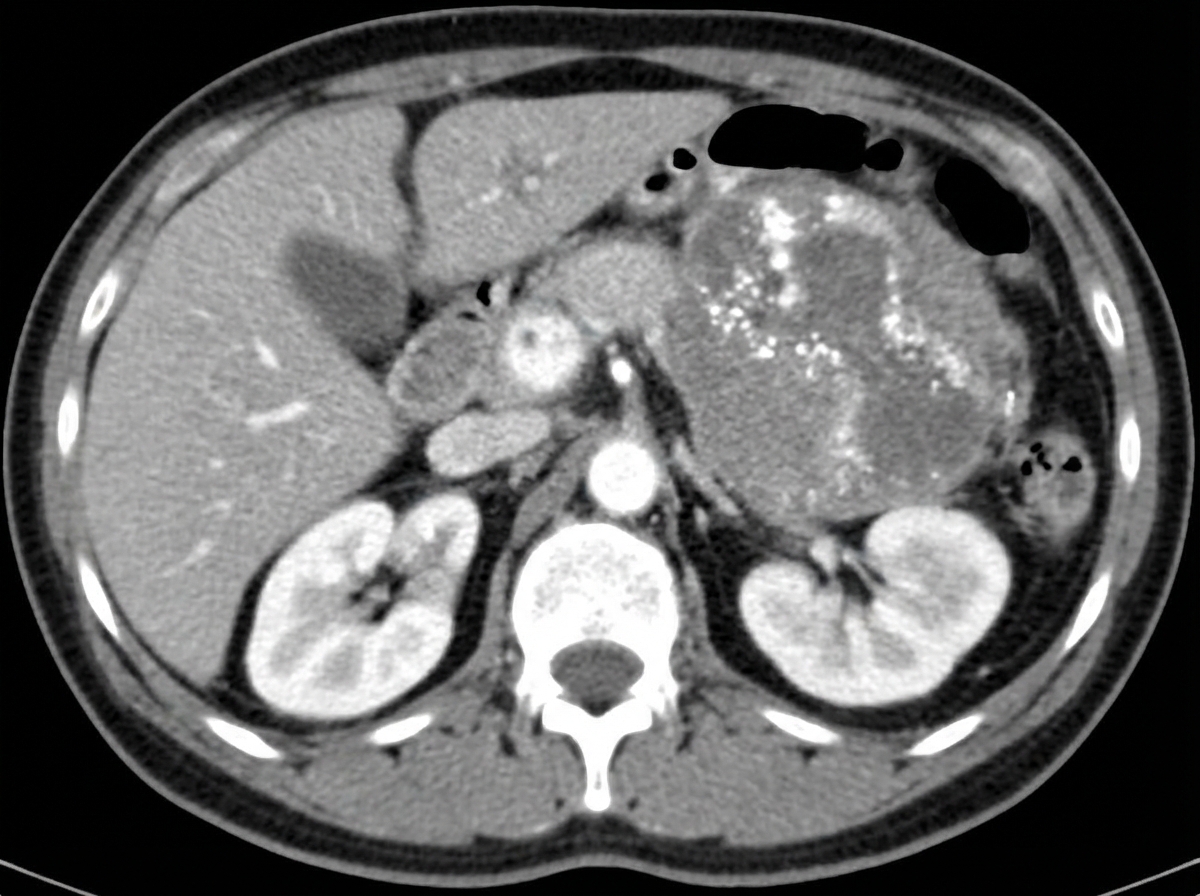
A 5-year-old child presents with a renal mass. Considering the most common cause in this age group, which of the following statements is not true?
What is the most common tumor of infancy?
What is the most common primary lung cancer in children?
Which of the following is NOT associated with Wilm's tumor?
Which of the following findings is not compatible with a diagnosis of juvenile myelomonocytic leukemia?
A child with Acute myeloid Leukemia presents with Hyperleukocytosis. Management includes all of the following, except:
Which of the following is the most common cause of a posterior mediastinum mass in children?
Wilm's tumor is associated with which of the following conditions?
What is the most common tumor of the small bowel in children?
What is the most likely diagnosis?
Practice by Chapter
Leukemias
Practice Questions
Lymphomas
Practice Questions
CNS Tumors
Practice Questions
Neuroblastoma
Practice Questions
Wilms Tumor
Practice Questions
Rhabdomyosarcoma
Practice Questions
Bone Tumors
Practice Questions
Retinoblastoma
Practice Questions
Histiocytosis Syndromes
Practice Questions
Principles of Pediatric Chemotherapy
Practice Questions
Hematopoietic Stem Cell Transplantation
Practice Questions
Late Effects of Cancer Treatment
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app