
Oncology — MCQs

On this page
A 9-year-old female child presents with a history of headache and visual disturbances. What is the most likely diagnosis?
Which of the following is the most common intracranial tumor in children?
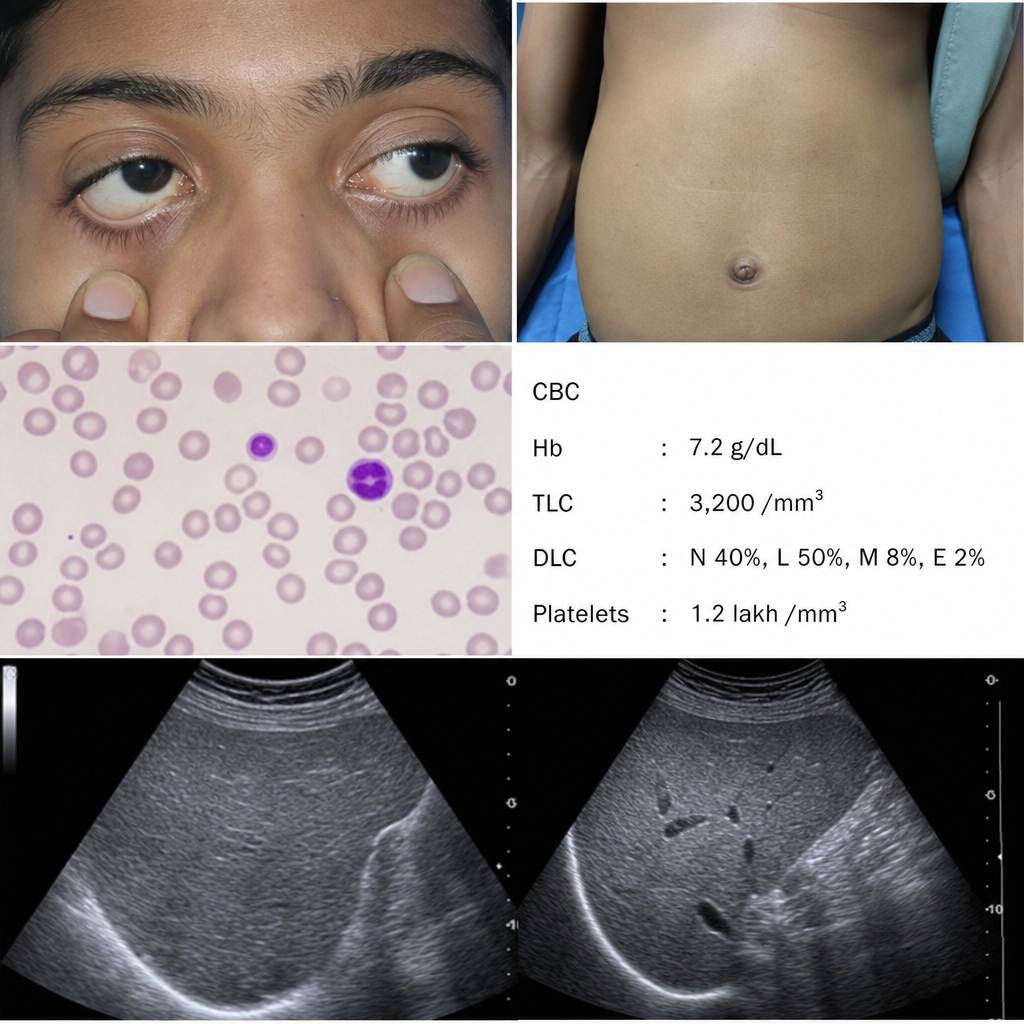
A child presents with the findings shown. The ultrasound confirms hepatomegaly (liver span >2 SD above normal for age). Which of the following findings are ALL present in this patient?
Which of the following is true about leukemia in Down's syndrome?
What is the commonest site of metastasis for Wilms' tumor?
What is the best prognostic factor for a 2-year-old child diagnosed with Acute Lymphoblastic Leukemia (ALL)?
Which of the following malignancies in children does not typically require immediate treatment?
An 8-year-old child is diagnosed with Langerhans cell histiocytosis with bone involvement. All of the following are true about Langerhans cell histiocytosis, EXCEPT:
A 7-year-old boy presents with a left renal mass, bone pain, and radiographically confirmed bone metastatic deposits. What is the most likely renal tumor?
Which of the following statements regarding Wilms tumor is false?
Practice by Chapter
Leukemias
Practice Questions
Lymphomas
Practice Questions
CNS Tumors
Practice Questions
Neuroblastoma
Practice Questions
Wilms Tumor
Practice Questions
Rhabdomyosarcoma
Practice Questions
Bone Tumors
Practice Questions
Retinoblastoma
Practice Questions
Histiocytosis Syndromes
Practice Questions
Principles of Pediatric Chemotherapy
Practice Questions
Hematopoietic Stem Cell Transplantation
Practice Questions
Late Effects of Cancer Treatment
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app