
Oncology — MCQs

On this page
Which is the most common malignancy in children?
A 6-year-old boy with lymphoreticular malignancy is scheduled for a cycle of chemotherapy. Which of the following investigations should be performed within the next 4 hours to diagnose tumor lysis syndrome?
Which of the following statements is false regarding Wilm's tumor?
What is the most common abdominal mass in children?
What is the most common site of metastasis in neuroblastoma?
A 5-year-old child presents with a history of fever off-and-on for the past 2 weeks, petechial spots all over the body, and increasing pallor for the past 1 month. Examination reveals splenomegaly 2 cm below the costal margin. What is the most likely diagnosis?
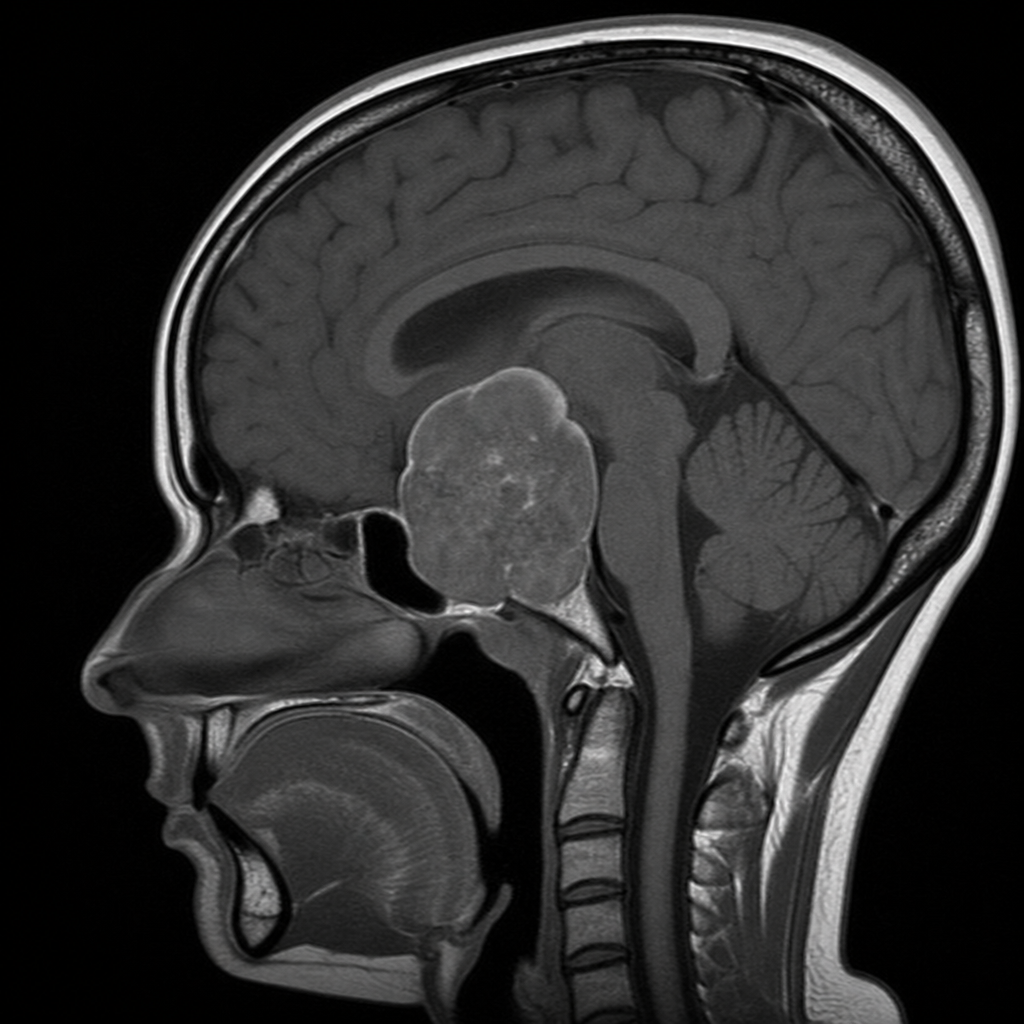
A 8-year-old boy presents with headache, a suprasellar mass, bitemporal hemianopia, and growth hormone deficiency. The MRI scan of his head is shown, demonstrating a cystic suprasellar mass with a calcified component. What is the diagnosis?
All of the following are good prognostic factors for childhood Acute Lymphoblastic Leukemia, except?
All of the following are good prognostic factors for childhood Acute Lymphoblastic Leukemia, except?
Which of the following are true about nephroblastoma except:
Practice by Chapter
Leukemias
Practice Questions
Lymphomas
Practice Questions
CNS Tumors
Practice Questions
Neuroblastoma
Practice Questions
Wilms Tumor
Practice Questions
Rhabdomyosarcoma
Practice Questions
Bone Tumors
Practice Questions
Retinoblastoma
Practice Questions
Histiocytosis Syndromes
Practice Questions
Principles of Pediatric Chemotherapy
Practice Questions
Hematopoietic Stem Cell Transplantation
Practice Questions
Late Effects of Cancer Treatment
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app