
Nephrology — MCQs

On this page
Which of the following is NOT true regarding Prune belly syndrome?
The neonatal kidney achieves concentrating ability equivalent to an adult's kidney by which age?
A child with recurrent urinary tract infections is most likely to show which of the following conditions?
What is the formula for calculating GFR?
Post-streptococcal glomerulonephritis in children is diagnosed by?
A 12-year-old boy presented with severe vomiting and diarrhea. He was brought to the hospital due to severe oliguria. He was given IV fluids and furosemide without any diuresis. Blood biochemistry revealed: Urea 120 mg% and serum creatinine 4 mg%. What is the most likely diagnosis?
A 4-month-old infant with a urinary tract infection (UTI) was treated for 14 days with IV cefotaxime. What is the next step in management?
A child presented with frothy urine, massive proteinuria, and edema. Urine examination revealed no RBCs, no WBCs, no casts, and no crystals. There is no prior episode of similar presentation. What is your diagnosis?
In Lowe syndrome, all of the following are seen except?
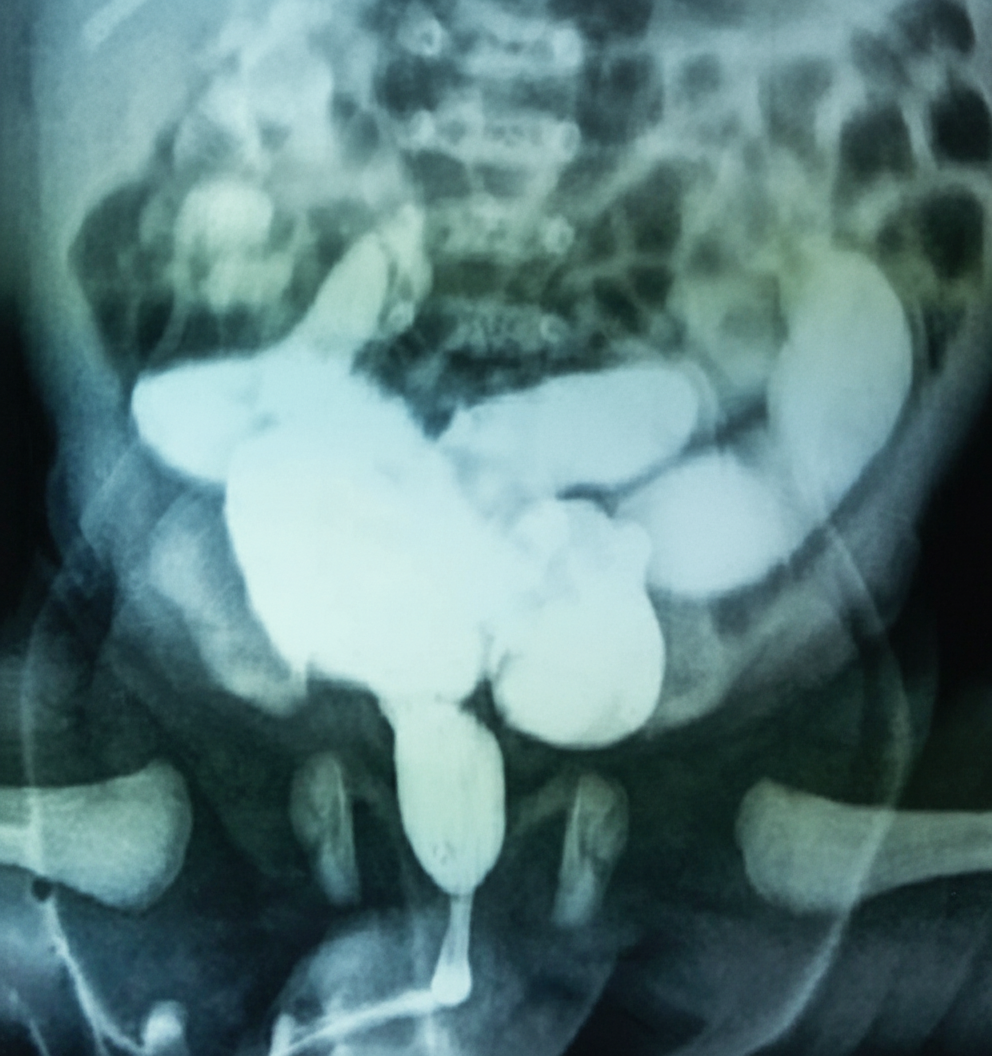
Physical examination of a neonate reveals a distended bladder and palpable kidneys. The infant produces a weak urinary stream. A voiding cystourethrogram is shown. He appears to be otherwise normal. Which of the following is the most likely diagnosis?
Practice by Chapter
Urinary Tract Infections
Practice Questions
Vesicoureteral Reflux
Practice Questions
Glomerulonephritis
Practice Questions
Nephrotic Syndrome
Practice Questions
Acute Kidney Injury
Practice Questions
Chronic Kidney Disease
Practice Questions
Renal Tubular Disorders
Practice Questions
Congenital Anomalies of the Kidney
Practice Questions
Hydronephrosis
Practice Questions
Hypertension in Children
Practice Questions
Hemolytic Uremic Syndrome
Practice Questions
Renal Replacement Therapy in Children
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app