
Nephrology — MCQs

On this page
Which of the following is a characteristic of a child with acute post-streptococcal glomerulonephritis?
What is the drug of choice for a child with a first episode of nephrotic syndrome?
A 6-year-old child has been drinking more water and urinating more frequently for the past 7 months. Physical examination reveals dehydration. Urinalysis findings include a pH of 6.5, specific gravity of 1.010, and no protein, blood, glucose, or ketones. There are no WBCs, RBCs, or casts. Serum electrolytes show Na+, 152 mmol/L; K+, 4.6 mmol/L; Cl-, 120 mmol/L; HCO3-, 21 mmol/L; urea nitrogen, 29 mg/dL; and creatinine, 3.2 mg/dL. An ultrasound scan shows bilaterally small kidneys with barely visible medullary cysts concentrated at the corticomedullary junction. Which of the following genes is most likely mutated in this child?
A 6-year-old child presents with malignant hypertension. What is the drug of choice?
Which is a reliable marker for estimating glomerular filtration rate (GFR) in children?
Which of the following is NOT a syndrome associated with renal disease?
A 5-year-old boy has a history of recurrent urinary tract infections. Urine cultures have grown Escherichia coli, Proteus mirabilis, and Enterococcus. Physical examination shows an abnormal constricted opening of the urethra on the ventral aspect of the penis, 1.5 cm from the tip of the glans penis. He also has a cryptorchid testis on the right and an inguinal hernia on the left. What term best describes the child's penile abnormality?
A feature of renal vasculitis in children is:
Pulmonary hypoplasia with urinary problems is associated with which of the following conditions?
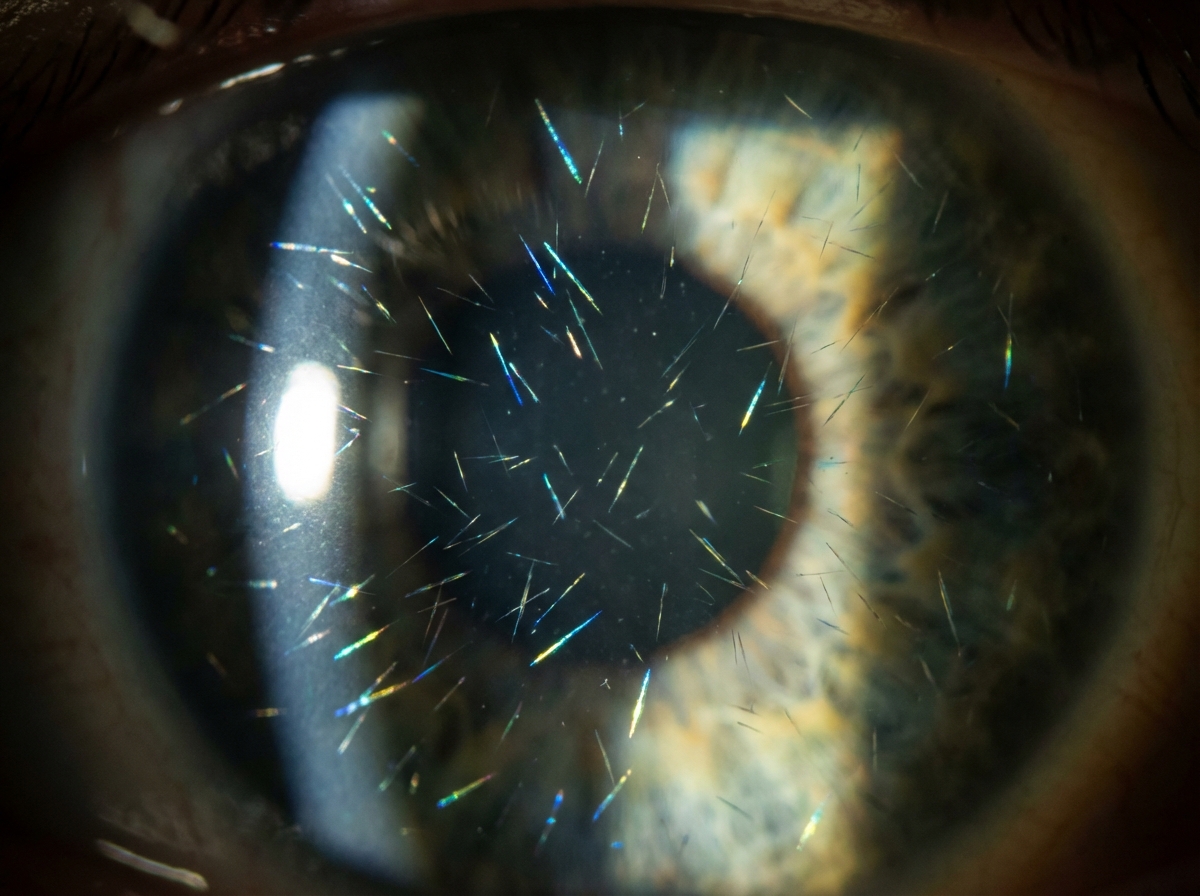
A child presented with polyuria, polydipsia, fever, and clinical features of rickets. Slit lamp examination shows specific findings. What is the probable diagnosis?
Practice by Chapter
Urinary Tract Infections
Practice Questions
Vesicoureteral Reflux
Practice Questions
Glomerulonephritis
Practice Questions
Nephrotic Syndrome
Practice Questions
Acute Kidney Injury
Practice Questions
Chronic Kidney Disease
Practice Questions
Renal Tubular Disorders
Practice Questions
Congenital Anomalies of the Kidney
Practice Questions
Hydronephrosis
Practice Questions
Hypertension in Children
Practice Questions
Hemolytic Uremic Syndrome
Practice Questions
Renal Replacement Therapy in Children
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app