
Nephrology — MCQs

On this page
A 9-year-old boy is brought with history of decreased urine output, cola colored urine and swelling of the face and hands, of 2 days duration. He is hypertensive, has a puffy face and pitting edema of the lower limbs. He has history of skin lesions 4 weeks earlier. A diagnosis of post streptococcal glomerulonephritis is made. ASO titers are likely to be?
Child with proteinuria, generalized edema, hypoproteinemia, and hyperlipidemia - most common cause is?
An infant with severe dehydration secondary to diarrhea suddenly presents with flank mass and blood in urine. The most probable diagnosis is?
A six year old male child presents to a hospital with recurrent gross hematuria for 2 years. There is no h/o burning micturition or pyuria. Urine routine examination demonstrated no pus cells and urine culture was sterile. Serum c3 levels were normal. What is the most Probable diagnosis -
A 7-year-old child with steroid dependent nephrotic syndrome has developed corticosteroid toxicity and posterior subcapsular cataracts. Which of the following is the best alternative for the treatment of the patient?
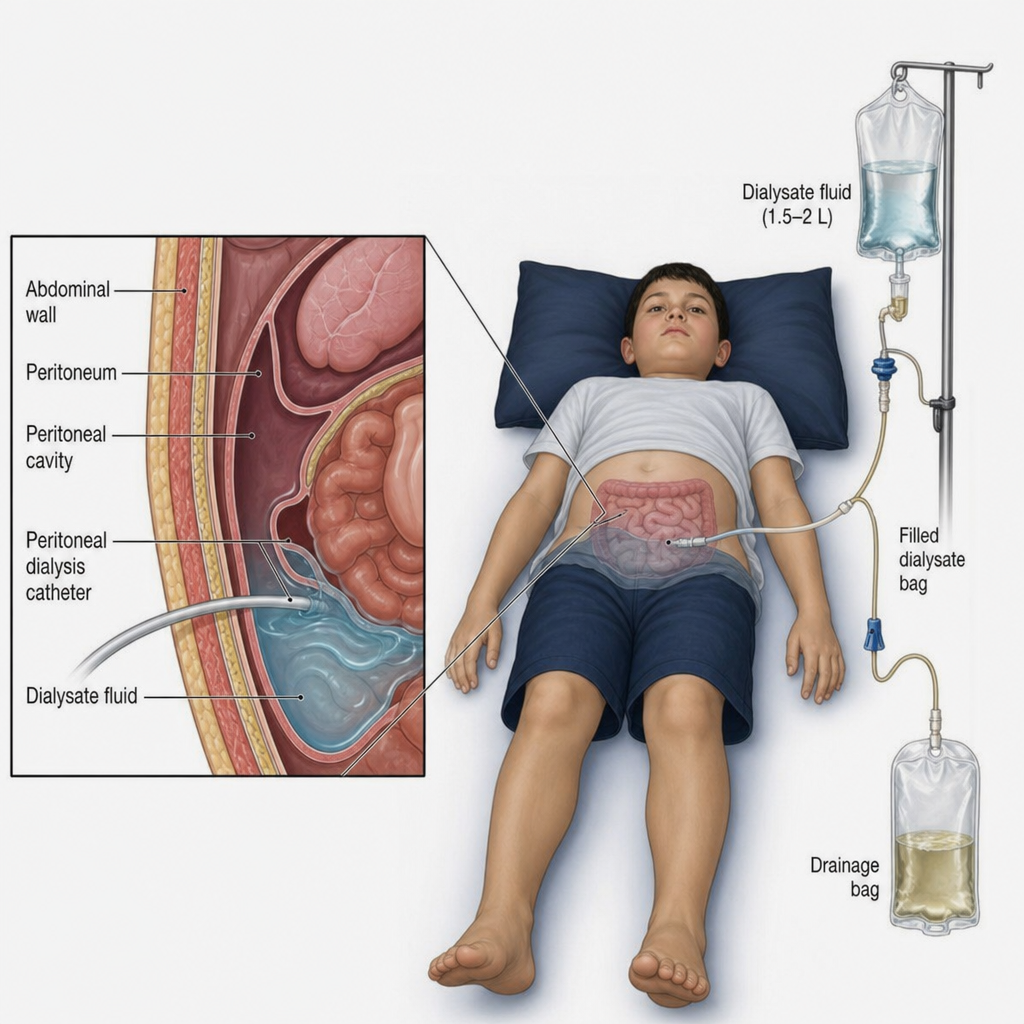
An 8-year-old child presented with a history of respiratory distress, altered sensorium & not passing urine for the last 15 hours. What is the procedure shown below that can be done as a part of emergency management of this child?
A child with nephrotic syndrome following an episode of diarrhea presented with acute kidney injury with a creatinine of 4.5. All of the following are possible reasons except?
A 5-month old formula fed infant has been brought with complaints of watery diarrhoea of 2 days duration and irritability of one day duration. He had been receiving WHO ORS at home. Physical examination reveals a markedly irritable child with a rather doughy skin and rapid pulse. The most likely diagnosis is-
An 8 years old child suffering from recurrent attacks of polyuria since childhood presents to the pediatrics OPD. On examination, the child has short stature. Vitals and B.P. are normal. S. Creatinine - 6 mg/dL, HCO3 - 16 meq/L, S Na+ - 134 meq/L. On USG, bilateral small kidneys are seen. Diagnosis is:
Most common cause of nephrotic syndrome in children?
Practice by Chapter
Urinary Tract Infections
Practice Questions
Vesicoureteral Reflux
Practice Questions
Glomerulonephritis
Practice Questions
Nephrotic Syndrome
Practice Questions
Acute Kidney Injury
Practice Questions
Chronic Kidney Disease
Practice Questions
Renal Tubular Disorders
Practice Questions
Congenital Anomalies of the Kidney
Practice Questions
Hydronephrosis
Practice Questions
Hypertension in Children
Practice Questions
Hemolytic Uremic Syndrome
Practice Questions
Renal Replacement Therapy in Children
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app