
Nephrology — MCQs

On this page
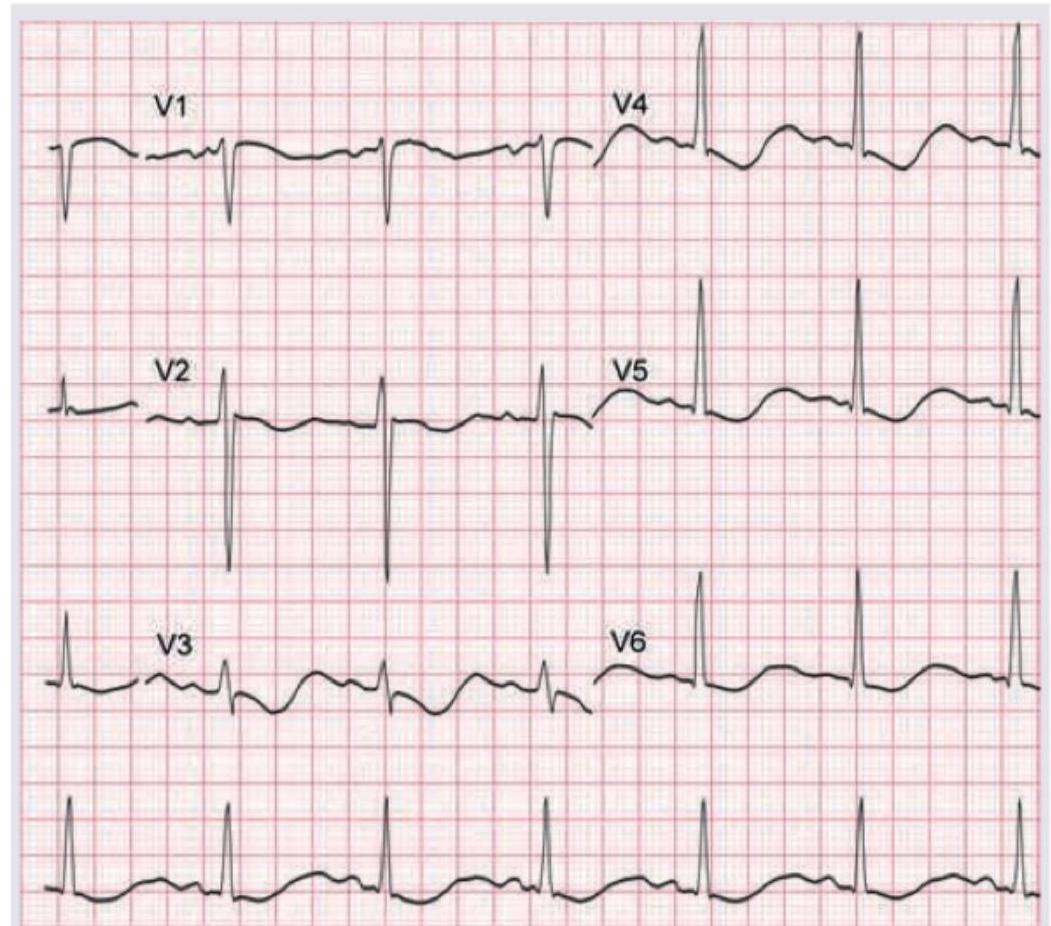
A 12-year-old child with renal tubular acidosis type I is having muscle cramps and weakness. ECG shows all except:
Which of the following statements are correct regarding management of hyperkalemia in a child? I. Intravenous calcium (gluconate or chloride) is given to enhance cellular uptake of potassium II. Beta adrenergic agonists (salbutamol or terbutaline) are used to stabilize myocardial cell membrane III. Regular insulin and glucose given intravenously enhance cellular uptake of potassium IV. Sodium polystyrene sulfonate enhances total body potassium elimination Select the answer using the code given below :
Which of the following statements are correct regarding hypernatremia in children? I. Diabetes insipidus due to a deficiency of antidiuretic hormone (ADH) may cause hypernatremia II. Addison disease may be associated with hypernatremia III. Use of boiled skimmed milk can lead to hypernatremia IV. Use of lactulose can lead to hypernatremia Select the answer using the code given below :
A 5-year-old boy is brought to the office by his mother with complaints of facial puffiness and “frothy” urine for 4 days. The puffiness first started in his eyes and then spread to the face. His mother does not provide any history of similar symptoms in the past. Past medical history is non-significant. His birth history is uneventful and all his vaccinations are up to date. The vital signs include: blood pressure 100/62 mm Hg, pulse 110/min, temperature 36.7°C (98.0°F), and respiratory rate 16/min. On examination, there is pitting edema of the upper and lower extremities bilaterally. Urinalysis results are as follows: pH 6.2 Color light yellow RBC none WBC 3–4/HPF Protein 4+ Cast Fat globules Glucose absent Crystal none Ketone absent Nitrite absent 24-hour urine protein excretion 4.1 g A renal biopsy is sent which shows normal glomeruli on light microscopy. Which of the following is the most likely diagnosis?
Treatment of choice used in nocturnal enuresis is:
A child presents with abdominal pain, arthralgia, hematuria, and hypertension. What is the diagnosis?
The most common underlying anomaly in a child with recurrent urinary tract infections is:
A breast fed child presents with hypernatremia (Serum sodium > 170m Eq/L). His urine sodium is 70 mEq/L. Which of the following is the most likely cause –
The following are causes of hematuria in childhood except
In Henoch–Schönlein purpura, renal involvement is generally not seen if there is no involvement by:
Practice by Chapter
Urinary Tract Infections
Practice Questions
Vesicoureteral Reflux
Practice Questions
Glomerulonephritis
Practice Questions
Nephrotic Syndrome
Practice Questions
Acute Kidney Injury
Practice Questions
Chronic Kidney Disease
Practice Questions
Renal Tubular Disorders
Practice Questions
Congenital Anomalies of the Kidney
Practice Questions
Hydronephrosis
Practice Questions
Hypertension in Children
Practice Questions
Hemolytic Uremic Syndrome
Practice Questions
Renal Replacement Therapy in Children
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app