
Neonatology — MCQs

On this page
What is the correct dose of i.v. adrenaline in term infants during neonatal resuscitation?
What is the recommended rate for blood transfusion in neonates?
A baby is born at 27 weeks of gestation and required mechanical ventilation for 4 weeks and CPAP for 1 week. He was maintained on room air subsequently. Based on the new definition of Bronchopulmonary Dysplasia (BPD), and assuming he remained on room air at 36 weeks post-menstrual age, what is the most appropriate classification of his condition?
Congenital varicella infection causes all except:
Prophylactic dose of vitamin K given to new born infants at delivery is?
What is the venous hematocrit level at which you will diagnose polycythemia in a newborn?
What will be the appropriate management for a very low birth weight preterm baby who is on a ventilator for respiratory distress and presents with clinical features of necrotizing enterocolitis with perforation?
Apgar score less than 3 at 5 minutes of life is a predictor of:
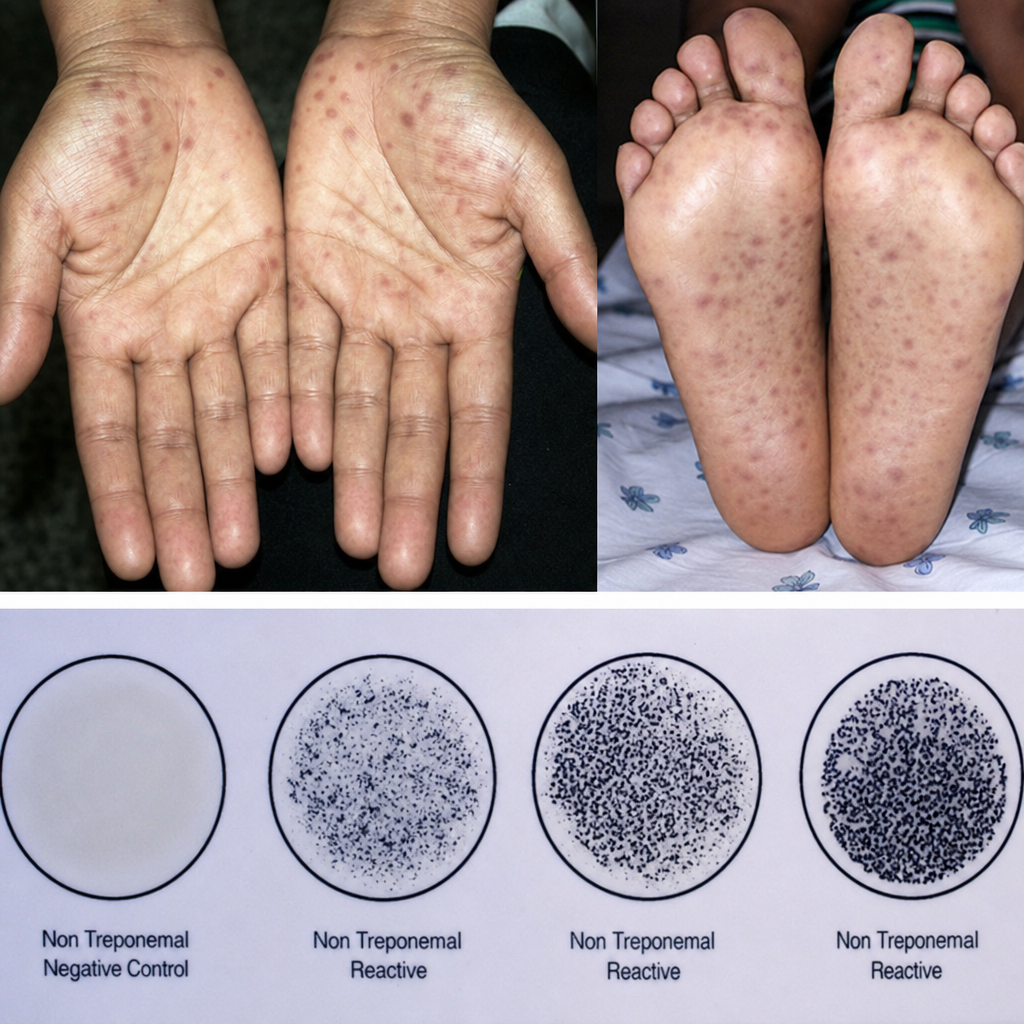
A 30-year-old pregnant female presented to the obstetrics OPD for the first time in the third trimester, at 36 weeks of gestation. She complained of fever, swollen lymph nodes, sore throat, and a characteristic rash on the palms as well as the soles of the feet. A serological screening test conducted in the given plate was positive for syphilis. Which of the following abnormalities can most likely be found in the child?
Infants of diabetic mothers manifest all of the following conditions except?
Practice by Chapter
Neonatal Resuscitation
Practice Questions
Care of the Normal Newborn
Practice Questions
Prematurity and Low Birth Weight
Practice Questions
Respiratory Distress Syndrome
Practice Questions
Neonatal Jaundice
Practice Questions
Neonatal Sepsis
Practice Questions
Necrotizing Enterocolitis
Practice Questions
Intraventricular Hemorrhage
Practice Questions
Persistent Pulmonary Hypertension
Practice Questions
Perinatal Asphyxia
Practice Questions
Neonatal Seizures
Practice Questions
Congenital Anomalies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app