
Neonatology — MCQs

On this page
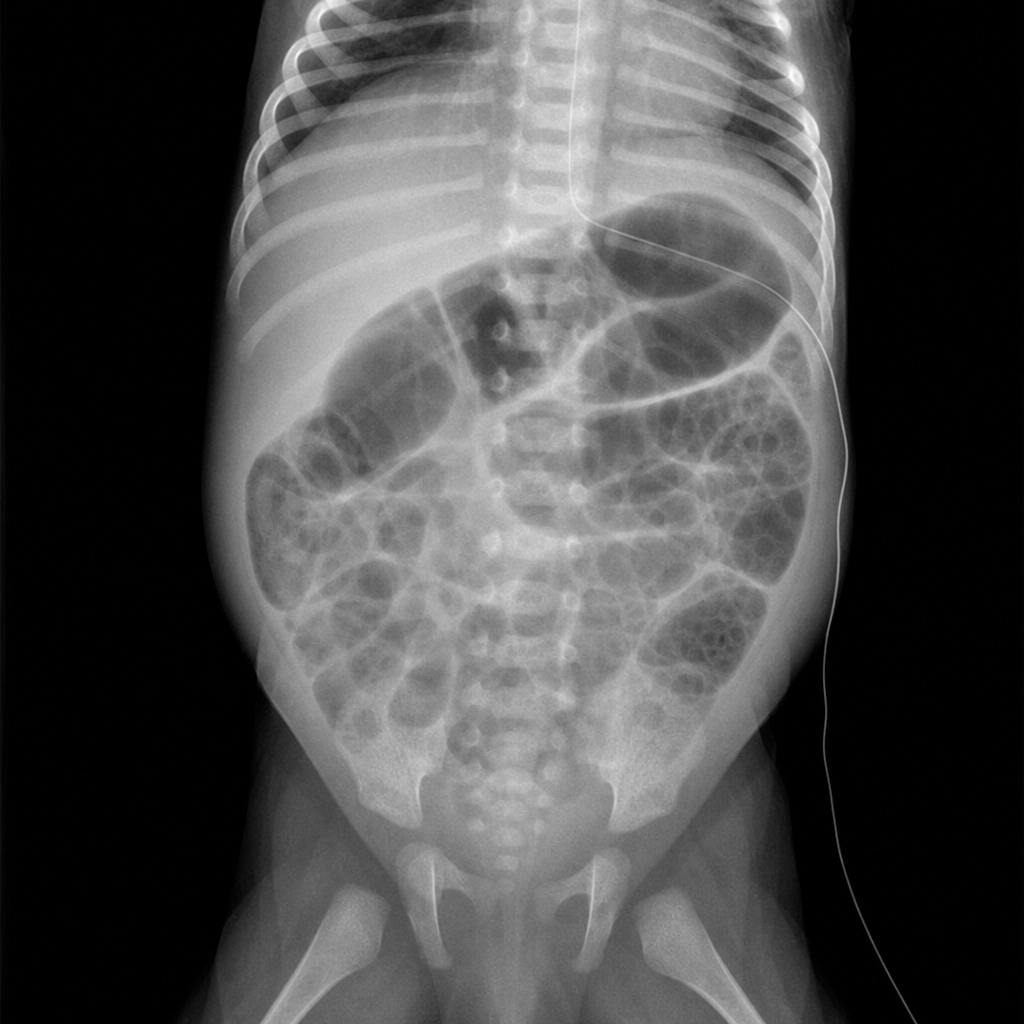
An 18-day-old newborn has difficulty feeding and diarrhea for 2 days. During this period he has vomited after each of his feeds. He was born at 28 weeks' gestation and weighed 1100-g (2-lb 7-oz). His feeds consist of breast milk and cow milk based-formula. He appears lethargic. His temperature is 36.4°C (97.5°F), pulse is 120/min, respirations are 67/min and blood pressure is 70/35 mm Hg. Examination shows diffuse abdominal tenderness; rigidity and guarding are present. Bowel sounds are absent. Test of the stool for occult blood is positive. His hemoglobin concentration is 12.8 g/dL, leukocyte count is 18,000/mm3 and platelet count is 78,000/mm3. An x-ray of the abdomen is shown. Which of the following is the most likely diagnosis?
A boy born vaginally in the 36th week of gestation to a 19-year-old woman (gravida 3, para 1) is assessed on his 2nd day of life. His vitals include: blood pressure is 85/40 mm Hg, pulse is 161/min, axillary temperature is 36.6°C (98.0°F), and respiratory rate is 44/min. He appears to be lethargic; his skin is jaundiced and slight acrocyanosis with several petechiae is noted. Physical examination reveals nystagmus, muffled heart sounds with a continuous murmur, and hepatosplenomegaly. The boy’s birth weight is 1.93 kg (4.25 lb) and Apgar scores at the 1st and 5th minutes were 5 and 8, respectively. His mother is unaware of her immunization status and did not receive any antenatal care. She denies any history of infection, medication use, or alcohol or illicit substance use during pregnancy. Serology for suspected congenital TORCH infection shows the following results: Anti-toxoplasma gondii IgM Negative Anti-toxoplasma gondii IgG Positive Anti-CMV IgM Negative Anti-CMV IgG Positive Anti-Rubella IgM Positive Anti-Rubella IgG Positive Anti-HSV IgM Negative Anti-HSV IgG Negative Which cardiac abnormality would be expected in this infant on echocardiography?
A patient at 37 weeks' gestation came to the hospital without antenatal check-up and presented with onset of labor. On examination, the mother is Hep B positive. What management should be given to the neonate?
A newborn loses maximum heat from:
Compression ventilation ratio in case of Neonatal CPR:
Differential cyanosis occurs in which of the following diseases:
Hypoglycemia in infants more than 24 hours of age is defined as blood glucose levels less than
The mother of this newborn had a vesicular varicella eruption near the time of delivery. What is this baby probably suffering from?

Which of the following cardiac defects can be seen in Congenital Rubella Syndrome?
The most characteristic manifestation of congenital toxoplasmosis is:
Practice by Chapter
Neonatal Resuscitation
Practice Questions
Care of the Normal Newborn
Practice Questions
Prematurity and Low Birth Weight
Practice Questions
Respiratory Distress Syndrome
Practice Questions
Neonatal Jaundice
Practice Questions
Neonatal Sepsis
Practice Questions
Necrotizing Enterocolitis
Practice Questions
Intraventricular Hemorrhage
Practice Questions
Persistent Pulmonary Hypertension
Practice Questions
Perinatal Asphyxia
Practice Questions
Neonatal Seizures
Practice Questions
Congenital Anomalies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app