
Neonatology — MCQs

On this page
Clinical features of an infant with Fetal growth retardation at birth include which of the following ? 1. Physical features give 'an old man look'. 2. Baby is alert, reflexes are normal. 3. Thick fat accumulates around shoulders of baby. Select the correct answer using the code given below :
Which of the following can be a complication in the baby due to post maturity of pregnancy ?
A 30-year-old female P2L2 had a forceps delivery 2 days back. There was injury to head of baby resulting in collection of blood in soft tissue between pericranium and flat bone of skull, limited by suture line. What is the probable diagnosis?
Which of the following is correct regarding "witch's milk"?
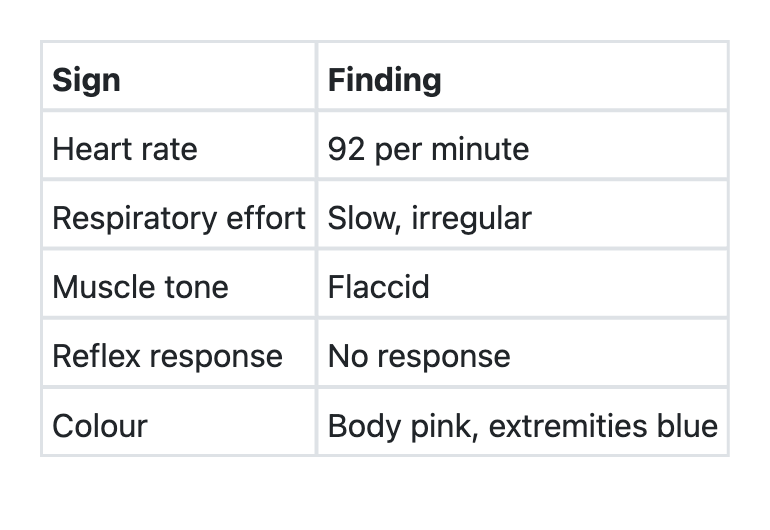
In a newborn, the Apgar score has been recorded at 1 minute of birth. Which one of the following best reflects the Apgar score of this newborn infant on a scale of 0 to 10?
To prevent neonatal tetanus in an infant born to a woman who has not been given Tetanus Toxoid (TT) appropriately during pregnancy, what should ideally be done?
Most common newborn rash which presents at 24-48 hours of life is
Apgar score is used in:
Meconium aspiration syndrome can be prevented by taking the following measures except :
A 37-week small-for-date neonate is most likely to develop
Practice by Chapter
Neonatal Resuscitation
Practice Questions
Care of the Normal Newborn
Practice Questions
Prematurity and Low Birth Weight
Practice Questions
Respiratory Distress Syndrome
Practice Questions
Neonatal Jaundice
Practice Questions
Neonatal Sepsis
Practice Questions
Necrotizing Enterocolitis
Practice Questions
Intraventricular Hemorrhage
Practice Questions
Persistent Pulmonary Hypertension
Practice Questions
Perinatal Asphyxia
Practice Questions
Neonatal Seizures
Practice Questions
Congenital Anomalies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app