
Neonatology — MCQs

On this page
Neonate born at 34 weeks with premature rupture of membranes develops respiratory distress. CXR shows a low-volume diffuse ground-glass reticulogranular pattern with air bronchograms. Which of the following is NOT part of the radiographic differential diagnosis?
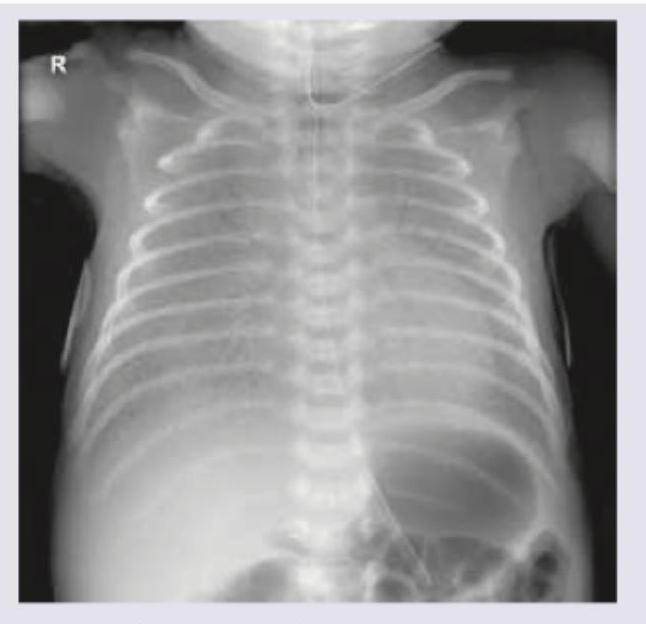
A term neonate presents with respiratory distress. The chest X-ray is shown below. Which of the following radiological findings is seen?

The image shows:
Which of the following is the first line of management of the condition shown?
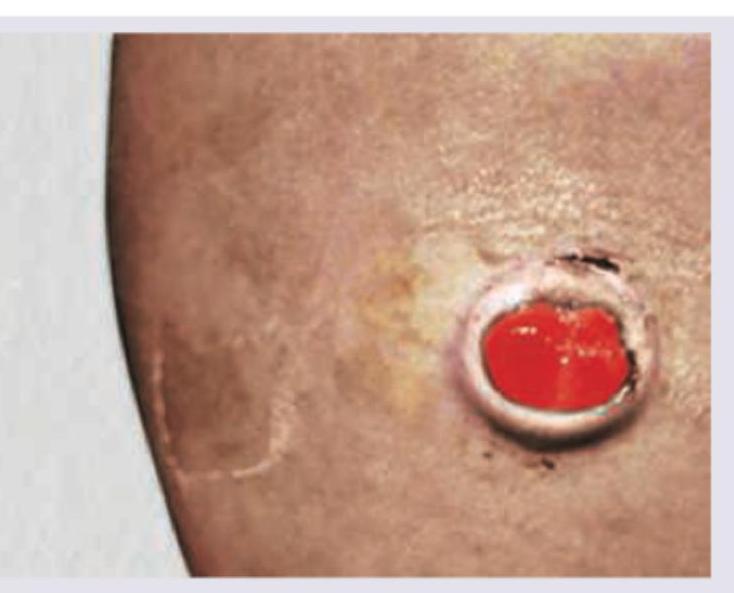
A 38-week gestational age newborn infant with a birth weight of 4.6 kg (>90th percentile for gestational age) is shown. The mother has a history of poorly controlled type 2 diabetes mellitus during pregnancy. What is the most likely diagnosis?

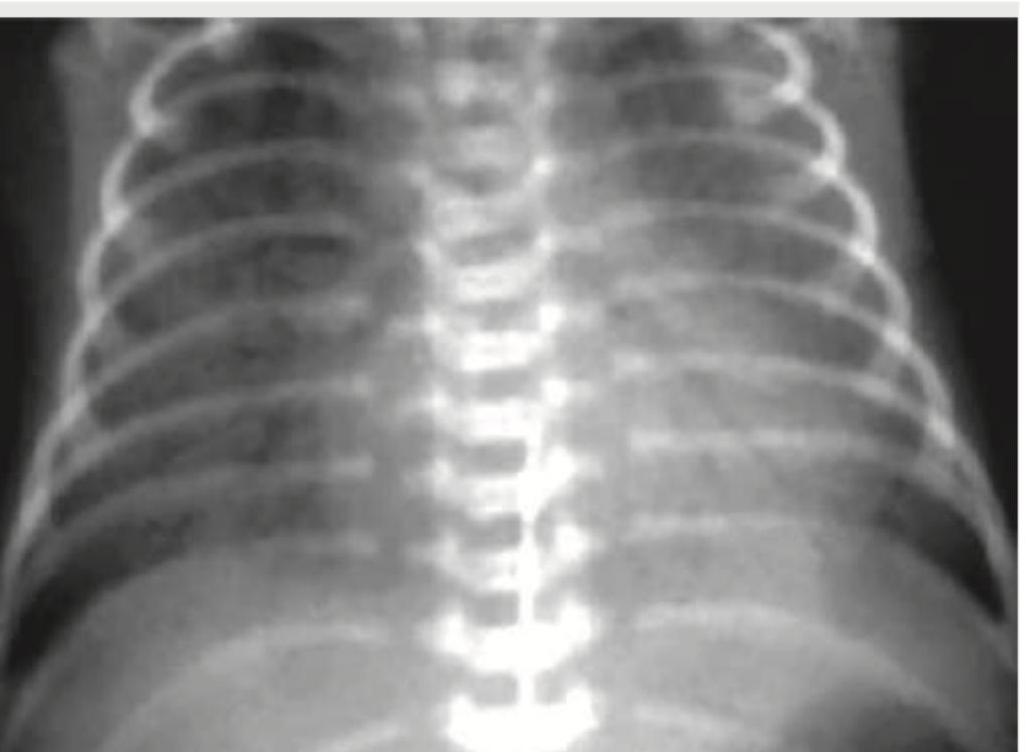
A 1-day-old neonate, born via home delivery, is brought with respiratory distress. The given CXR shows:
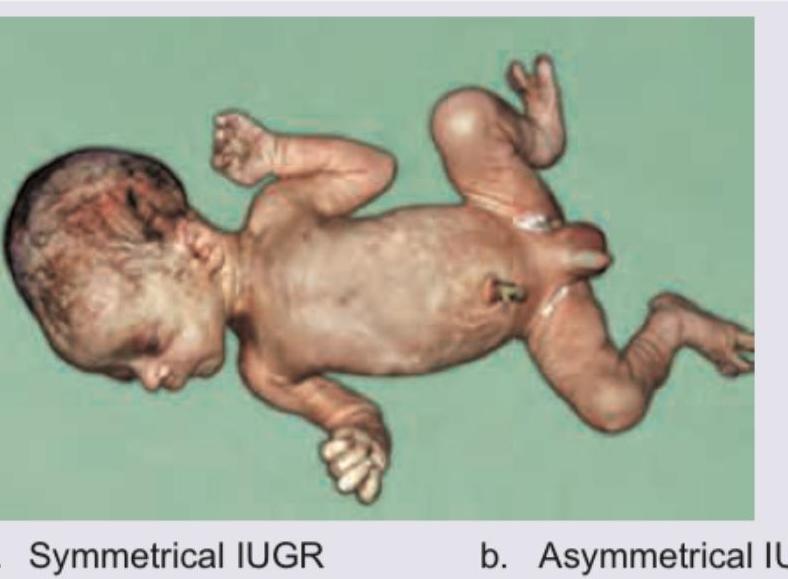
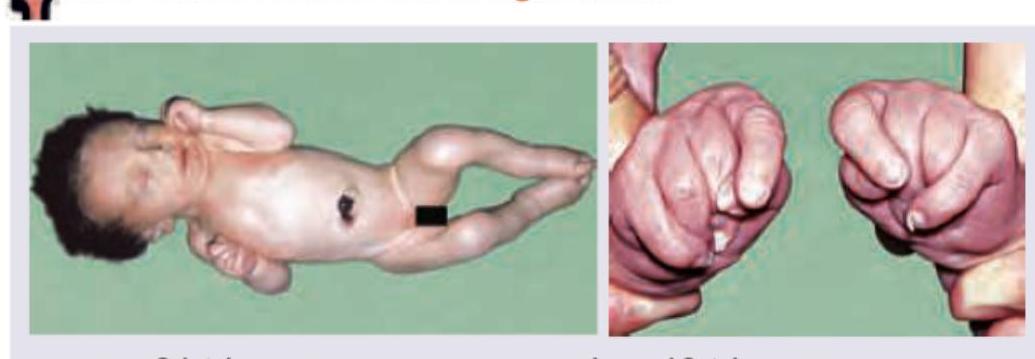
A newborn presents with the clinical features shown in the image below. What is the most likely diagnosis?
"Small for Date" (SFD) babies, also known as "small for gestational age" babies, weigh less than what percentile for the gestational age?
Which of the following are neonatal complications of maternal diabetes during pregnancy? I. Hyperbilirubinemia II. Hypocalcemia III. Cardiomyopathy IV. Hypoglycemia Select the correct answer using the code given below :
A term baby with birth weight of 2.8 kg is born to a primigravida mother through vaginal delivery and cried immediately after birth. Which of the following statements are correct regarding his initial care after birth ? I. The baby should be initiated on breastfeeding within one hour of birth II. The baby should be kept in a separate area from the mother III. The baby should be administered with 0.5 mg of vitamin K intramuscularly IV. The baby should be thoroughly examined for congenital malformations from head to toe Select the answer using the code given below :
Practice by Chapter
Neonatal Resuscitation
Practice Questions
Care of the Normal Newborn
Practice Questions
Prematurity and Low Birth Weight
Practice Questions
Respiratory Distress Syndrome
Practice Questions
Neonatal Jaundice
Practice Questions
Neonatal Sepsis
Practice Questions
Necrotizing Enterocolitis
Practice Questions
Intraventricular Hemorrhage
Practice Questions
Persistent Pulmonary Hypertension
Practice Questions
Perinatal Asphyxia
Practice Questions
Neonatal Seizures
Practice Questions
Congenital Anomalies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app