
Neonatology — MCQs

On this page
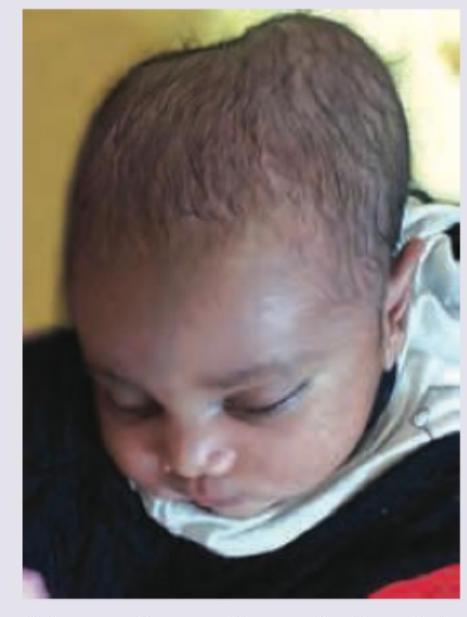
All are true about the swelling on scalp of a 2-day old neonate except: (Recent NEET Pattern 2016-17)
A 2-day-old neonate presents with plethora, jitteriness, poor feeding, and respiratory distress. Venous hematocrit is measured at 72%. What investigations and management are indicated in the condition shown in the image?

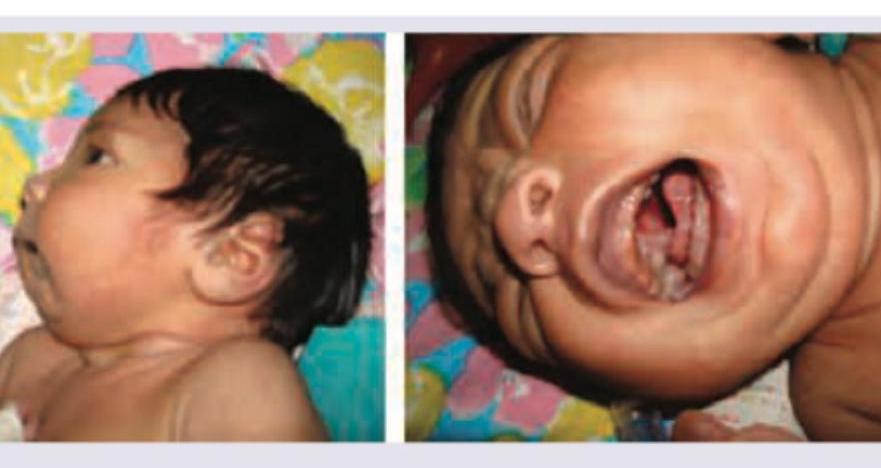
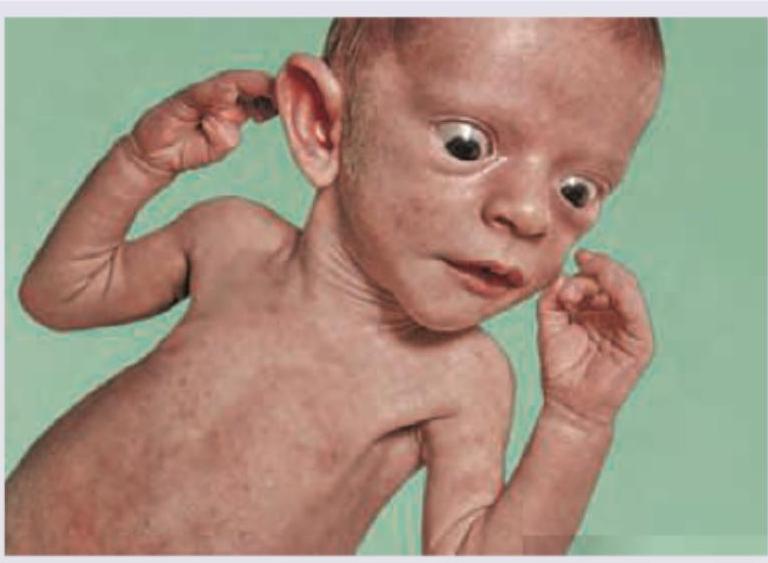
A 2-week-old neonate presents with feeding problems and otitis media. Based on the clinical image, what is the most likely diagnosis?
A 2-day-old neonate under phototherapy unit. For exchange transfusion serum bilirubin-albumin ratio should be: (Recent NEET Pattern 2016-17)
A newborn presents with macrosomia, plethoric appearance, and increased subcutaneous fat. The image shows:

Mother of a 6-hour-old neonate has pointed to passage of stool of the following color. Which of the following best describes the clinical possibility?

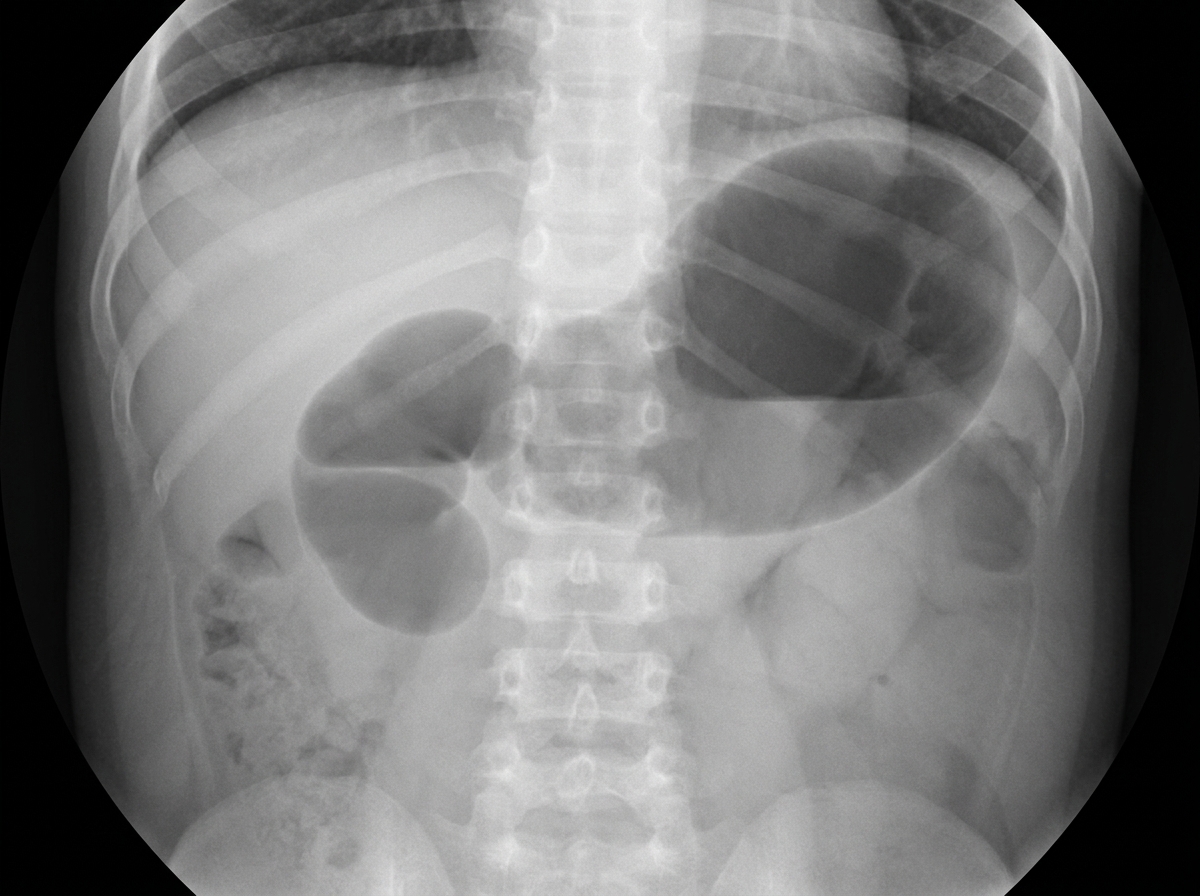
Child has not passed stool by 2nd day of life. X-Ray study done shows:
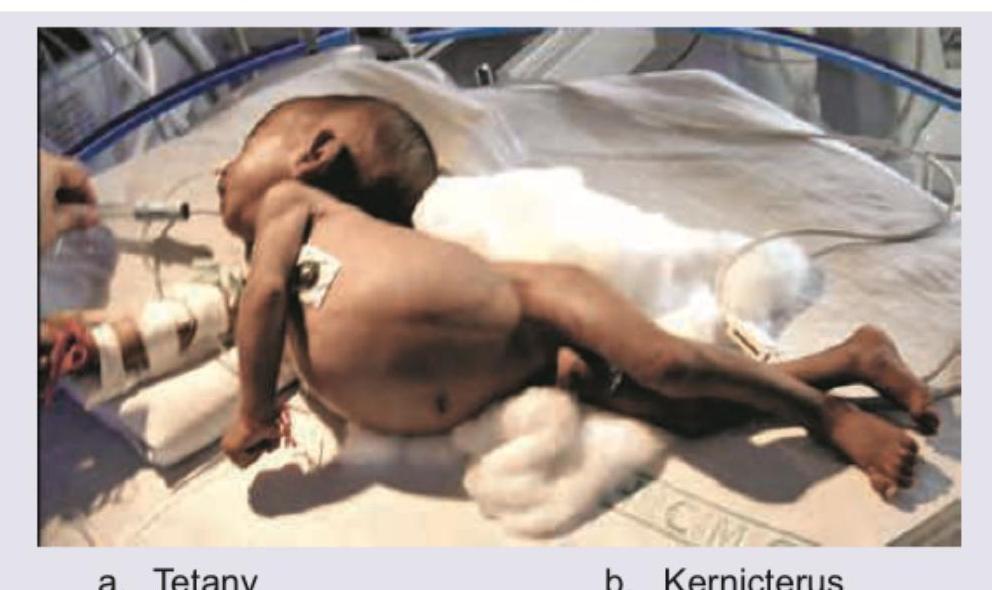
Which of the following diseases can lead to the position shown in the image?
Which of the following is the best diagnosis of this neonate who is excessively hungry, warm with flushed skin?
Preterm child on cow milk due to death of mother is having blood in stools. X-ray abdomen was done. Which radiological sign is demonstrated on the abdominal radiograph?

Practice by Chapter
Neonatal Resuscitation
Practice Questions
Care of the Normal Newborn
Practice Questions
Prematurity and Low Birth Weight
Practice Questions
Respiratory Distress Syndrome
Practice Questions
Neonatal Jaundice
Practice Questions
Neonatal Sepsis
Practice Questions
Necrotizing Enterocolitis
Practice Questions
Intraventricular Hemorrhage
Practice Questions
Persistent Pulmonary Hypertension
Practice Questions
Perinatal Asphyxia
Practice Questions
Neonatal Seizures
Practice Questions
Congenital Anomalies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app