
Neonatology — MCQs

On this page
A newborn immediately after delivery has the lesion shown in the image. The lesion is:

The following image shows:
Which of the following interventions is being done in this neonate?

A 3-week-old infant is brought to the clinic. The umbilical cord stump separated at 2 weeks of age. Since then, a small lesion has persisted at the umbilicus with mild serous discharge but no feculent or urinary drainage. There is no history of foul odor or passage of gas from the umbilicus. What is the best treatment for the lesion shown in the figure?

The pictured neonate was born to a mother with diabetes. All are true about the image shown except:

The mother is concerned about the whitish material in the groin of the child. Which is incorrect?

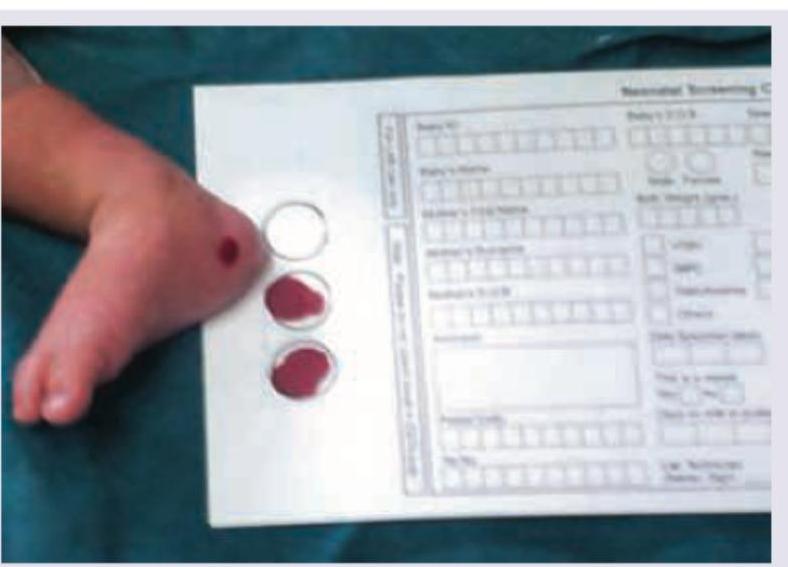
Which blood-collection procedure is shown in the following image performed in a neonate?
A term neonate born at 38 weeks gestation with a birth weight at the 3rd percentile is shown in the image. All are true about the image shown except:

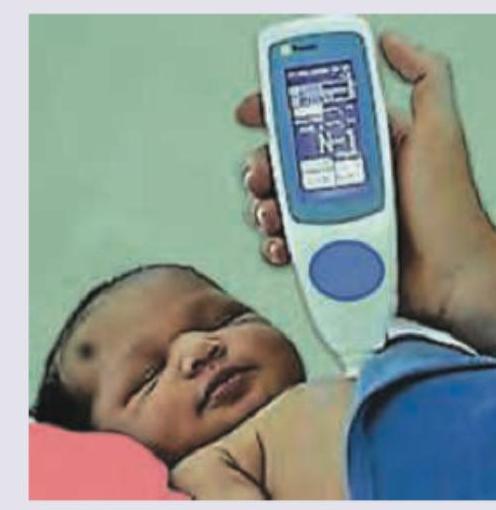
What test is being performed on this neonate in the NICU?

The following appearance of a child can occur in which of the following situations:

Practice by Chapter
Neonatal Resuscitation
Practice Questions
Care of the Normal Newborn
Practice Questions
Prematurity and Low Birth Weight
Practice Questions
Respiratory Distress Syndrome
Practice Questions
Neonatal Jaundice
Practice Questions
Neonatal Sepsis
Practice Questions
Necrotizing Enterocolitis
Practice Questions
Intraventricular Hemorrhage
Practice Questions
Persistent Pulmonary Hypertension
Practice Questions
Perinatal Asphyxia
Practice Questions
Neonatal Seizures
Practice Questions
Congenital Anomalies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app