
Neonatology — MCQs

On this page
What is the daily fluid requirement for a 3-day-old baby with a birth weight of 1500 grams?
A neonate was brought with a history of frothiness from the mouth and respiratory distress. An X-ray of the neonate is given below. What is the diagnosis?
How much oxygen is given to a term infant with respiratory distress during resuscitation?
A neonate delivered at 36-week gestation develops respiratory distress soon after birth. CXR is as shown. Likely diagnosis?
Which of the following best explains the mechanism of breast milk jaundice?
Positive pressure ventilation (PPV) in neonatal resuscitation is indicated in all of the following except:
A neonate is being resuscitated as shown in the image. What is the ratio of chest compressions:rescue breaths for this patient?

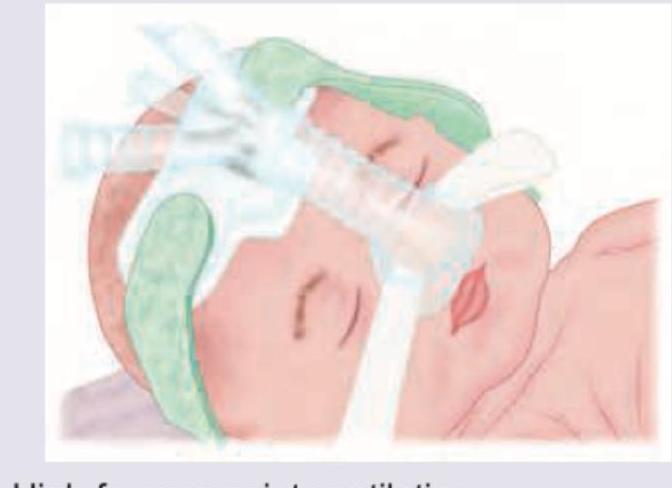
What ventilation modality is shown below?
A child presents in the first week of life with recurrent vomiting, failure to thrive. On examination enlarged liver and spleen are palpated. Blood work shows hyperlipidemia and deranged LFT. CT abdomen was performed. What is the clinical diagnosis?

A 2-hour-old neonate born by normal vaginal delivery has a scalp swelling that was present at birth, is soft and pitting in texture, crosses suture lines, has not progressed since delivery, and the neonate has stable vital signs. What is the probable cause?

Practice by Chapter
Neonatal Resuscitation
Practice Questions
Care of the Normal Newborn
Practice Questions
Prematurity and Low Birth Weight
Practice Questions
Respiratory Distress Syndrome
Practice Questions
Neonatal Jaundice
Practice Questions
Neonatal Sepsis
Practice Questions
Necrotizing Enterocolitis
Practice Questions
Intraventricular Hemorrhage
Practice Questions
Persistent Pulmonary Hypertension
Practice Questions
Perinatal Asphyxia
Practice Questions
Neonatal Seizures
Practice Questions
Congenital Anomalies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app