
Neonatology — MCQs

On this page
What is the most important indicator of successful neonatal resuscitation?
The late features of kernicterus include all of the following except:
Which of the following is NOT a common complication in a neonate born to a mother with diabetes mellitus?
What is the most common causative organism for neonatal septicemia?
What is the APGAR score of a newborn presenting with cyanosis, heart rate of 70 beats per minute, hypotonia, and grimacing in response to nasal suction?
A 26-year-old multigravida mother delivered a male baby weighing 4.2 kg at 37 weeks of gestation via emergency cesarean section for obstructed labor. One hour after birth, the child developed respiratory distress. He was kept nil per os (NPO) and received intravenous fluids. He maintained oxygen saturation on room air. No antibiotics were administered. A chest radiograph revealed fluid in the interlobar fissure. The respiratory distress resolved by 24 hours of life. What is the most likely diagnosis?
CSF examination in a one-day-old term male infant with convulsions reveals cell count -- 10 RBCs/HPF, 50 cells; protein -- 70 mg/dl; sugar -- 30 mg/dl. Blood sugar is 40 mg/dl. What is the most likely diagnosis?
A mother diagnosed with chickenpox delivered a healthy, afebrile, term infant 7 days ago. What is the most appropriate management step for the infant?
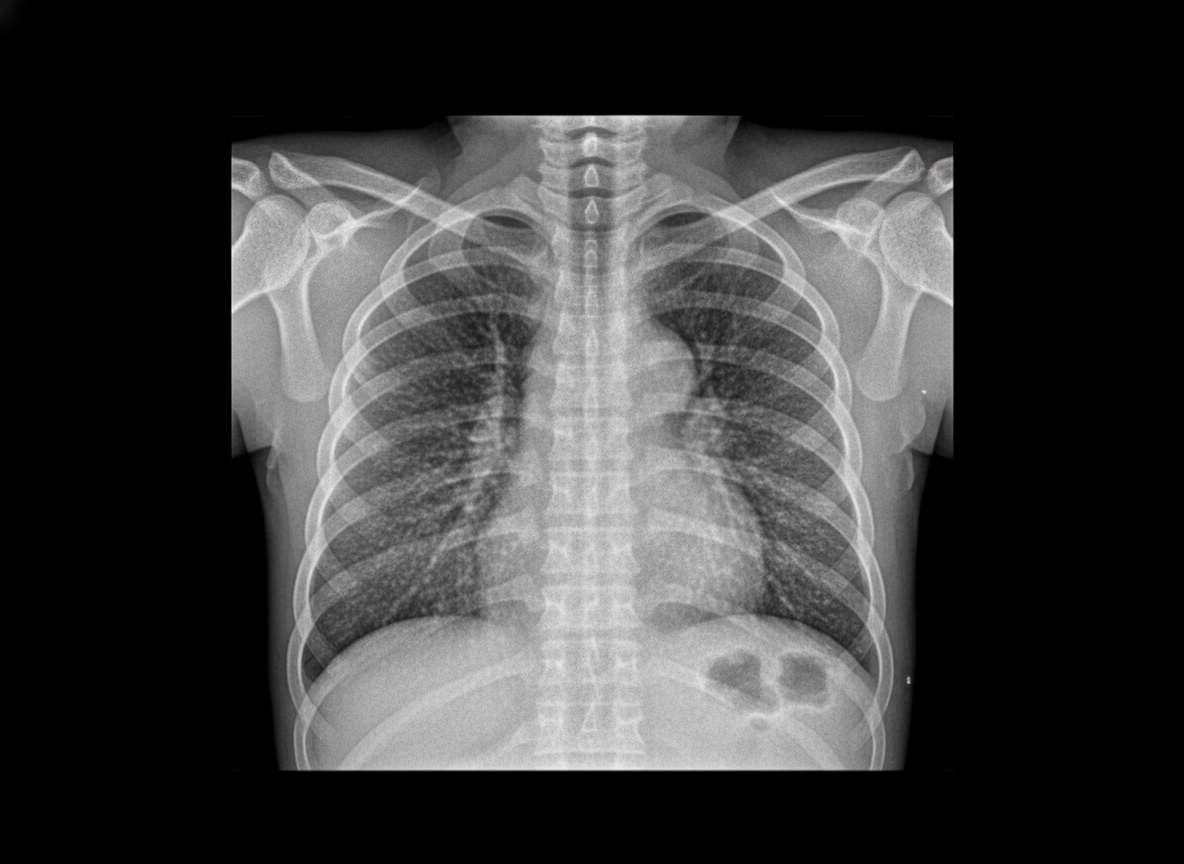
An 8-hour-old term infant develops increased respiratory distress, hypothermia, and hypotension. A complete blood count (CBC) demonstrates a white blood cell (WBC) count of 2500/µL with 80% bands. The chest radiograph is shown below. Which of the following is the most likely diagnosis?

An 8-hour-old term infant develops increased respiratory distress, hypothermia, and hypotension. A complete blood count (CBC) demonstrates a white blood cell (WBC) count of 2500/mL with 80% bands. The chest radiograph is shown below. Which of the following is the most likely diagnosis?
Practice by Chapter
Neonatal Resuscitation
Practice Questions
Care of the Normal Newborn
Practice Questions
Prematurity and Low Birth Weight
Practice Questions
Respiratory Distress Syndrome
Practice Questions
Neonatal Jaundice
Practice Questions
Neonatal Sepsis
Practice Questions
Necrotizing Enterocolitis
Practice Questions
Intraventricular Hemorrhage
Practice Questions
Persistent Pulmonary Hypertension
Practice Questions
Perinatal Asphyxia
Practice Questions
Neonatal Seizures
Practice Questions
Congenital Anomalies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app