
Neonatology — MCQs

On this page
Which of the following situations correctly indicates when alcohol-based hand rub (rather than soap-and-water handwashing) is preferred before entering a NICU?
What is the blood glucose level considered hyperglycemia in a neonate?
Which of the following is best for the transport of a newborn while maintaining body temperature?
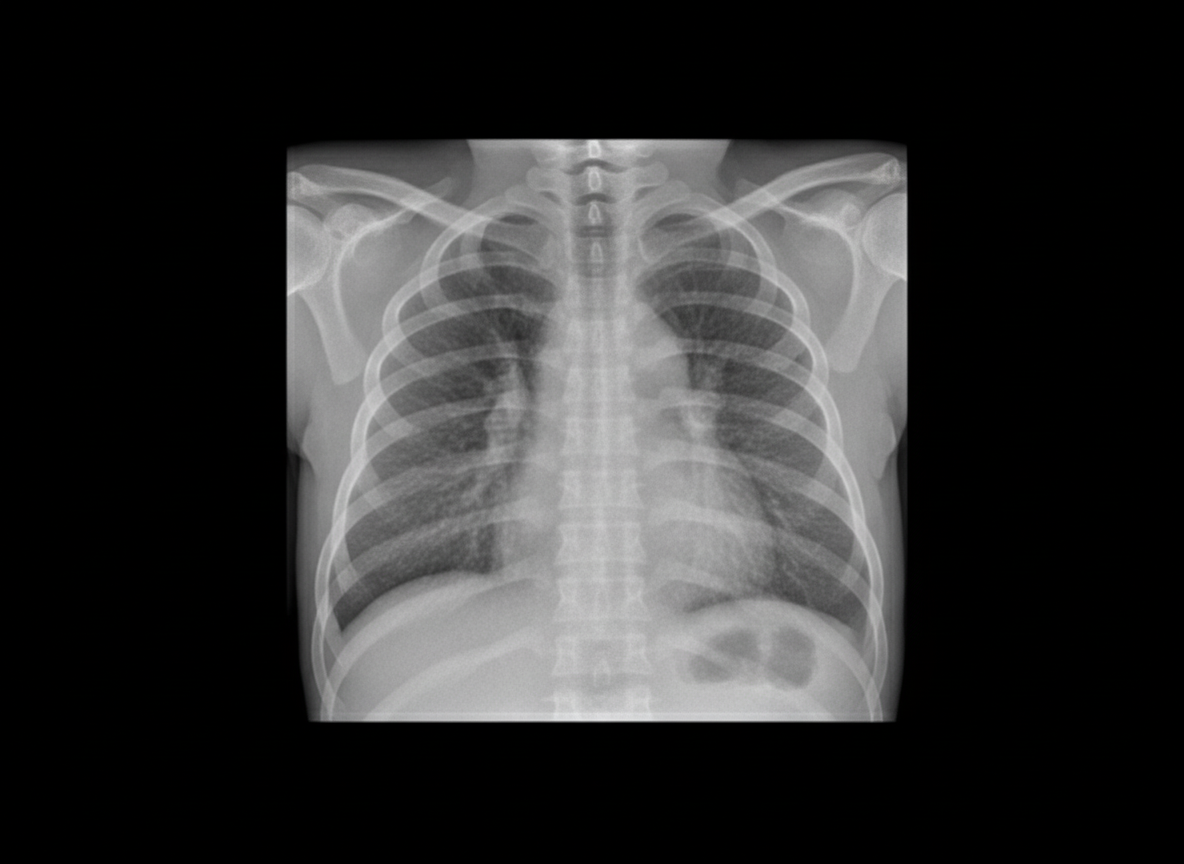
A neonate born at 34 weeks gestation with premature rupture of membranes undergoes a chest X-ray. Which of the following is LEAST likely to be considered in the differential diagnosis of the findings on the chest X-ray?
A 40-year-old man developed burning pain and paresthesias of his left scalp and forehead for 9 days. Three days later, he noted several papules on his scalp, followed the next day by more on his forehead over the left eyebrow and on his left upper eyelid. These evolved into small blisters on which crusts formed. As the older lesions became crusted, new papules appeared in the same general area. Examination revealed several erythematous papules, and groups of clear-fluid-filled vesicles with erythematous bases, and crusted papules in the left anterior scalp, forehead, and upper eyelid. The tip of the nose was spared. If this same condition affects a pregnant female in the 1st trimester, which of the following abnormalities can be seen in the newborn?
With reference to Respiratory Distress Syndrome (RDS), all of the following statements are true EXCEPT:
A 28-year-old woman gave birth to a small for gestational age newborn at 38 weeks of pregnancy. On examination, the newborn was found to have rhinitis, a distended abdomen, wrinkled skin, and palmoplantar blisters. The woman had an earlier history of abortion and stillbirth. What is the most likely diagnosis?
Which of the following skin changes in a newborn disappear spontaneously?
A premature baby of 34 weeks gestation was delivered and developed bullous lesions on the skin. Radiographs show periostitis. What should be the next investigation?
IUGR is characterized by all EXCEPT?
Practice by Chapter
Neonatal Resuscitation
Practice Questions
Care of the Normal Newborn
Practice Questions
Prematurity and Low Birth Weight
Practice Questions
Respiratory Distress Syndrome
Practice Questions
Neonatal Jaundice
Practice Questions
Neonatal Sepsis
Practice Questions
Necrotizing Enterocolitis
Practice Questions
Intraventricular Hemorrhage
Practice Questions
Persistent Pulmonary Hypertension
Practice Questions
Perinatal Asphyxia
Practice Questions
Neonatal Seizures
Practice Questions
Congenital Anomalies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app