
Neonatology — MCQs

On this page
A 30-hour-old breastfed infant develops jaundice affecting the face, palms, and soles. Which of the following is NOT a cause of this presentation?
Pharmacological closure of patent ductus arteriosus in a premature infant is by administration of ______________?
What is the minimum number of pustules required to diagnose a possible severe bacterial infection in children?
What is the definition of extreme preterm?
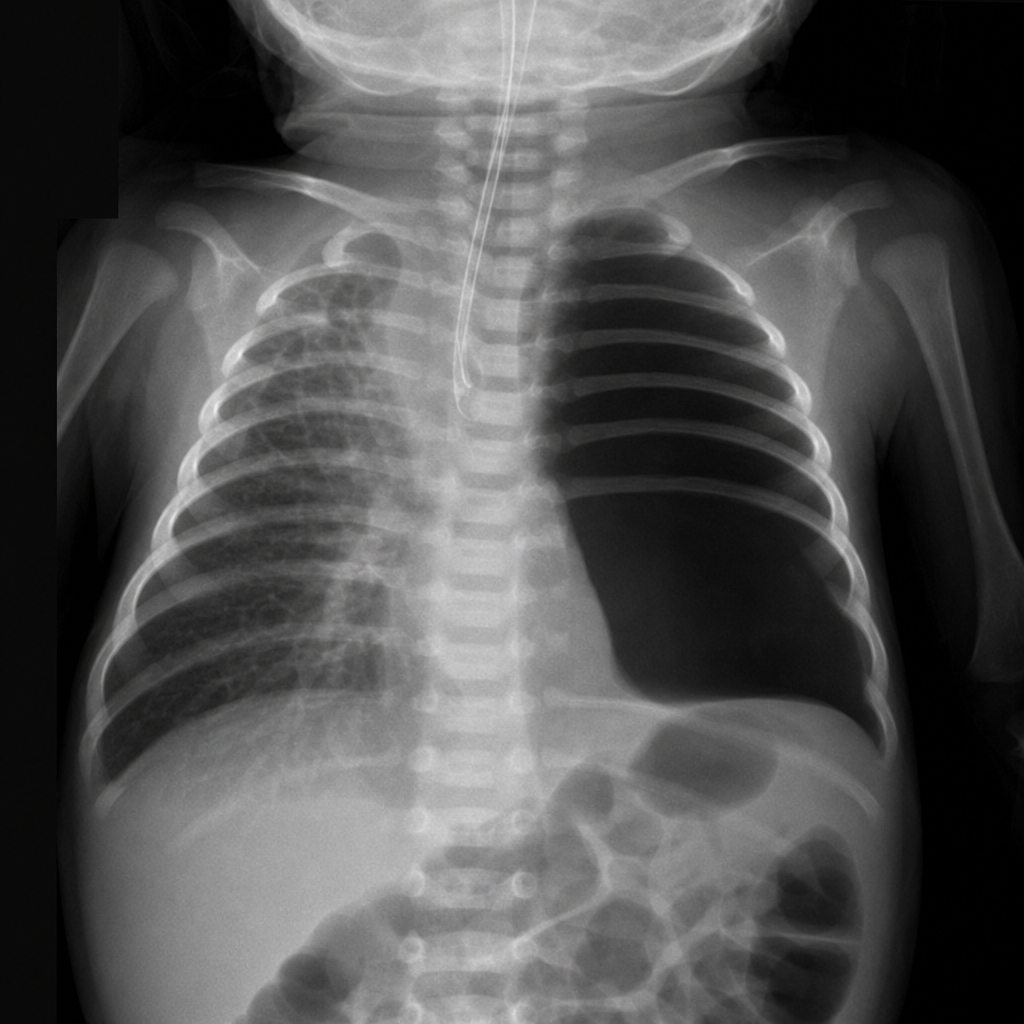
A newborn infant develops respiratory distress immediately after birth. The infant's abdomen is scaphoid. No breath sounds are heard on the left side of the chest, but they are audible on the right. Bowel sounds are heard in the left chest. Intubation is successful with little or no improvement in clinical status. An emergency chest x-ray is shown. Which of the following is the most likely explanation for this infant's condition?
All of the following are accepted therapeutic measures initiated in hyperammonemic states in an infant except?
Meconium ileus is associated with all of the following except?
Late onset hemorrhagic disease of the newborn is characterized by all of the following features except?
A 6-hour-old infant delivered with difficulty by low forceps exhibits an asymmetric Moro reflex involving the right arm. The infant is cyanotic and has labored respiration. The abdomen does not bulge with inspiration, and breath sounds are decreased in the right chest. What is the most likely diagnosis?
A 30-week gestation, 1.2 kg infant develops respiratory distress, grunting, and chest retractions within 2 hours of birth. His respiratory rate is 70/min. What is the MOST appropriate next step in management?
Practice by Chapter
Neonatal Resuscitation
Practice Questions
Care of the Normal Newborn
Practice Questions
Prematurity and Low Birth Weight
Practice Questions
Respiratory Distress Syndrome
Practice Questions
Neonatal Jaundice
Practice Questions
Neonatal Sepsis
Practice Questions
Necrotizing Enterocolitis
Practice Questions
Intraventricular Hemorrhage
Practice Questions
Persistent Pulmonary Hypertension
Practice Questions
Perinatal Asphyxia
Practice Questions
Neonatal Seizures
Practice Questions
Congenital Anomalies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app