
Neonatology — MCQs

On this page
All of the following decrease the risk of necrotizing enterocolitis (NEC) except?
Maternal rubella infection during pregnancy can cause all of the following in the newborn EXCEPT:
In neonatal cholestasis, what is the threshold for elevated direct bilirubin?
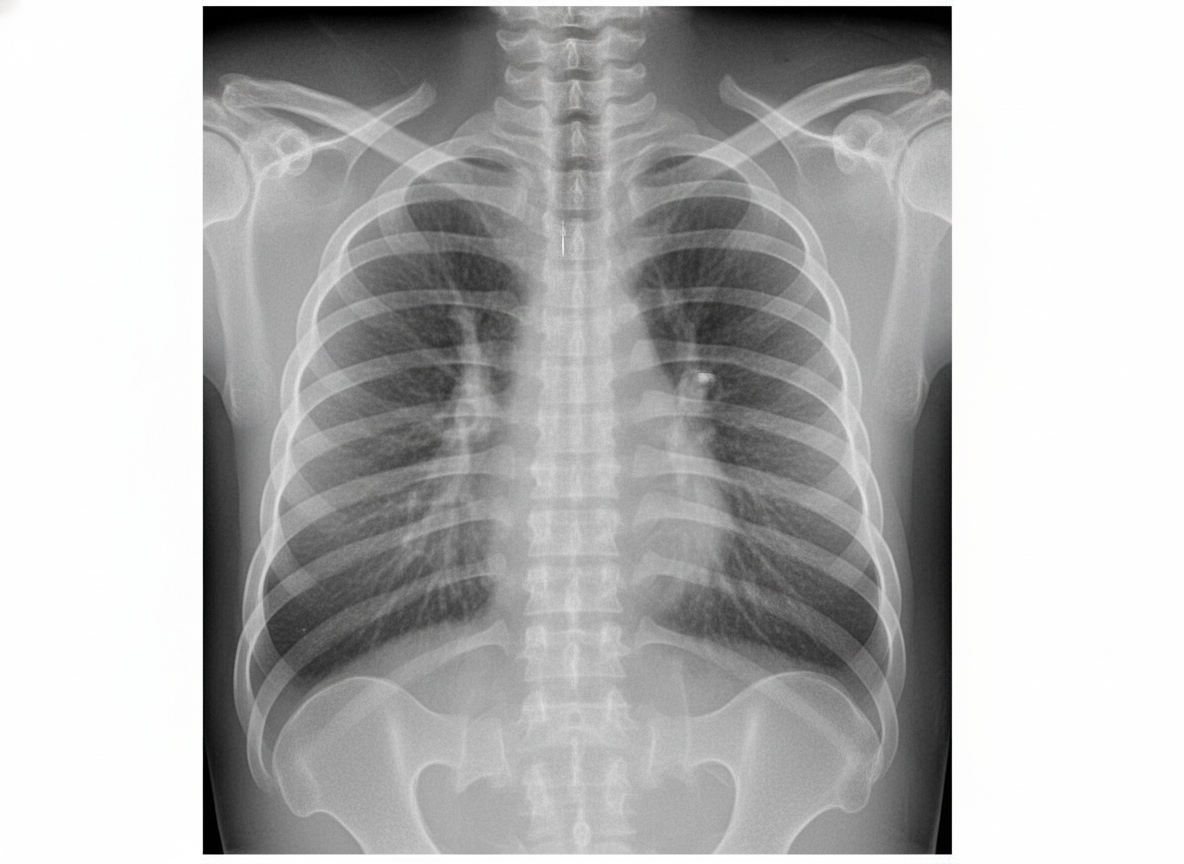
A term neonate presents with mild respiratory distress soon after birth. Chest X-ray shows typical findings. How is this condition managed?
What is a common injury to a neonate during birth?
Two weeks after birth, a neonate develops sepsis, skin vesicles, and conjunctivitis. Over the next several days, the baby's condition deteriorates with the development of seizures, cranial nerve palsies, and lethargy. The baby dies approximately one week after the onset of symptoms. Which of the following infectious agents would most likely cause this clinical presentation?
Which of the following is NOT useful in the management of meconium aspiration syndrome?
A baby is considered large for gestational age (LGA) if their birth weight is:
A syndrome of multiple congenital anomalies including microcephaly, cardiac anomalies, and growth retardation has been described in children of women who are heavy users of which substance?
A term newborn infant is noticed to be hypotonic. Which of the following is a possible diagnosis?
Practice by Chapter
Neonatal Resuscitation
Practice Questions
Care of the Normal Newborn
Practice Questions
Prematurity and Low Birth Weight
Practice Questions
Respiratory Distress Syndrome
Practice Questions
Neonatal Jaundice
Practice Questions
Neonatal Sepsis
Practice Questions
Necrotizing Enterocolitis
Practice Questions
Intraventricular Hemorrhage
Practice Questions
Persistent Pulmonary Hypertension
Practice Questions
Perinatal Asphyxia
Practice Questions
Neonatal Seizures
Practice Questions
Congenital Anomalies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app