
Neonatology — MCQs

On this page
All are true about breast milk jaundice except:
Which of the following causes can result in an infant being large for gestational age, EXCEPT?
What is the weight range for a Low Birth Weight (LBW) baby?
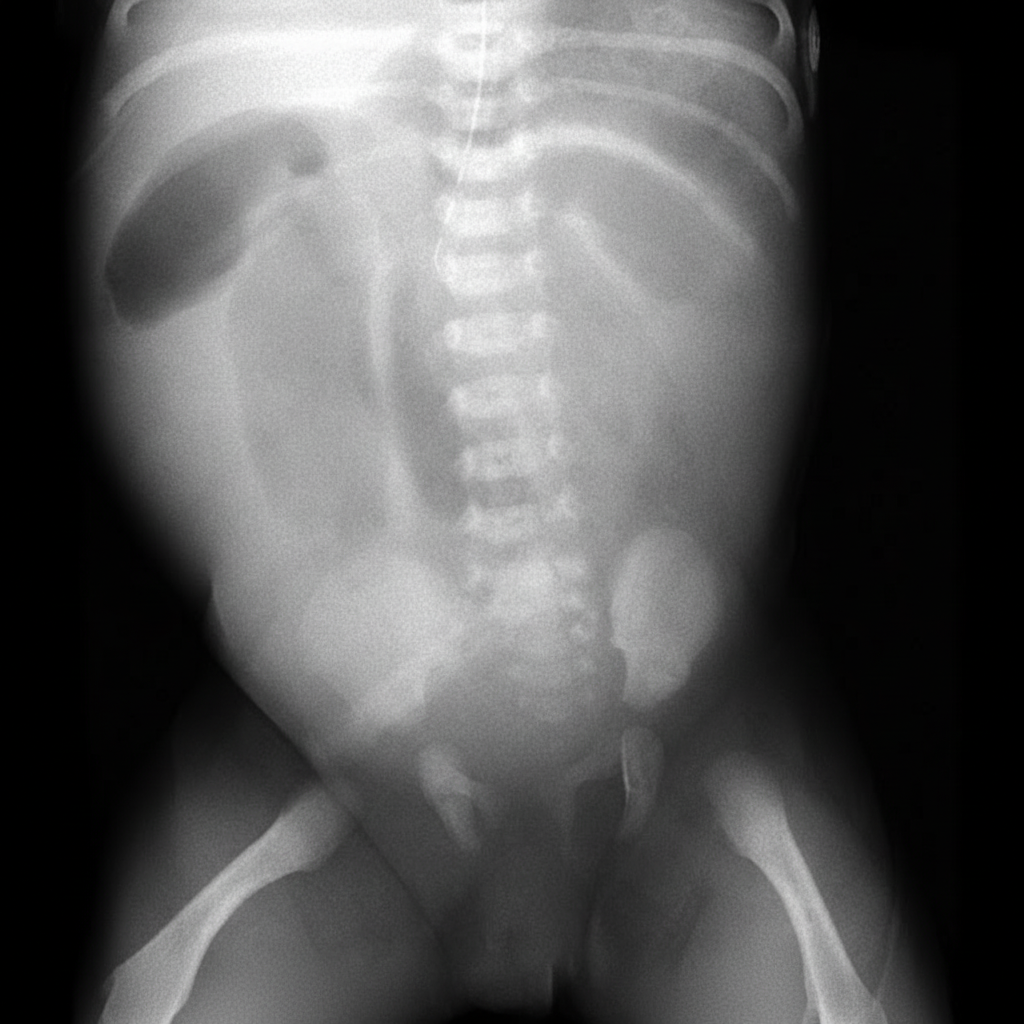
A 1-day-old baby boy has developed abdominal distension and bilious emesis. Prenatal history was significant for areas of echogenic bowel seen on ultrasound. An abdominal radiograph and contrast enema were performed; the contrast enema demonstrated a microcolon with inspissated meconium in the distal ileum. Based on these findings, what underlying disease should be suspected?
Collection of sero-sanguineous fluid in the scalp is known as what?
What is the drug of choice for neonatal seizures?
Edema of hands and feet in infants is characterized by which of the following conditions?
A 20-day-old infant presents with fever and irritability. Fontanelles are bulging and neck stiffness is present. Which of the following is the commonest cause of meningitis in the postneonatal period?
A female infant is born approximately 10 weeks prematurely (at 30 weeks) and weighs 1710 gm. She has respiratory distress syndrome and is treated with exogenous surfactant. She is intubated endotracheally with mechanical ventilation immediately after birth. Over the first 4 days after birth, the ventilator pressure and the fraction of inspired oxygen are reduced. Beginning on the fifth day after birth, she has brief desaturations that become more persistent. She needs increased ventilator and oxygen support on the seventh day after birth. She becomes cyanotic. Further examination, echocardiogram, and x-rays reveal left atrial enlargement, an enlarged pulmonary artery, increased pulmonary vasculature, and a continuous machine-like murmur. Which of the following is the most likely diagnosis?
A 3-month-old boy is brought to the physician because his parents cannot find one of his testicles. Physical examination confirms the parents' observation. Which of the following is the most likely diagnosis?
Practice by Chapter
Neonatal Resuscitation
Practice Questions
Care of the Normal Newborn
Practice Questions
Prematurity and Low Birth Weight
Practice Questions
Respiratory Distress Syndrome
Practice Questions
Neonatal Jaundice
Practice Questions
Neonatal Sepsis
Practice Questions
Necrotizing Enterocolitis
Practice Questions
Intraventricular Hemorrhage
Practice Questions
Persistent Pulmonary Hypertension
Practice Questions
Perinatal Asphyxia
Practice Questions
Neonatal Seizures
Practice Questions
Congenital Anomalies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app