
Neonatology — MCQs

On this page
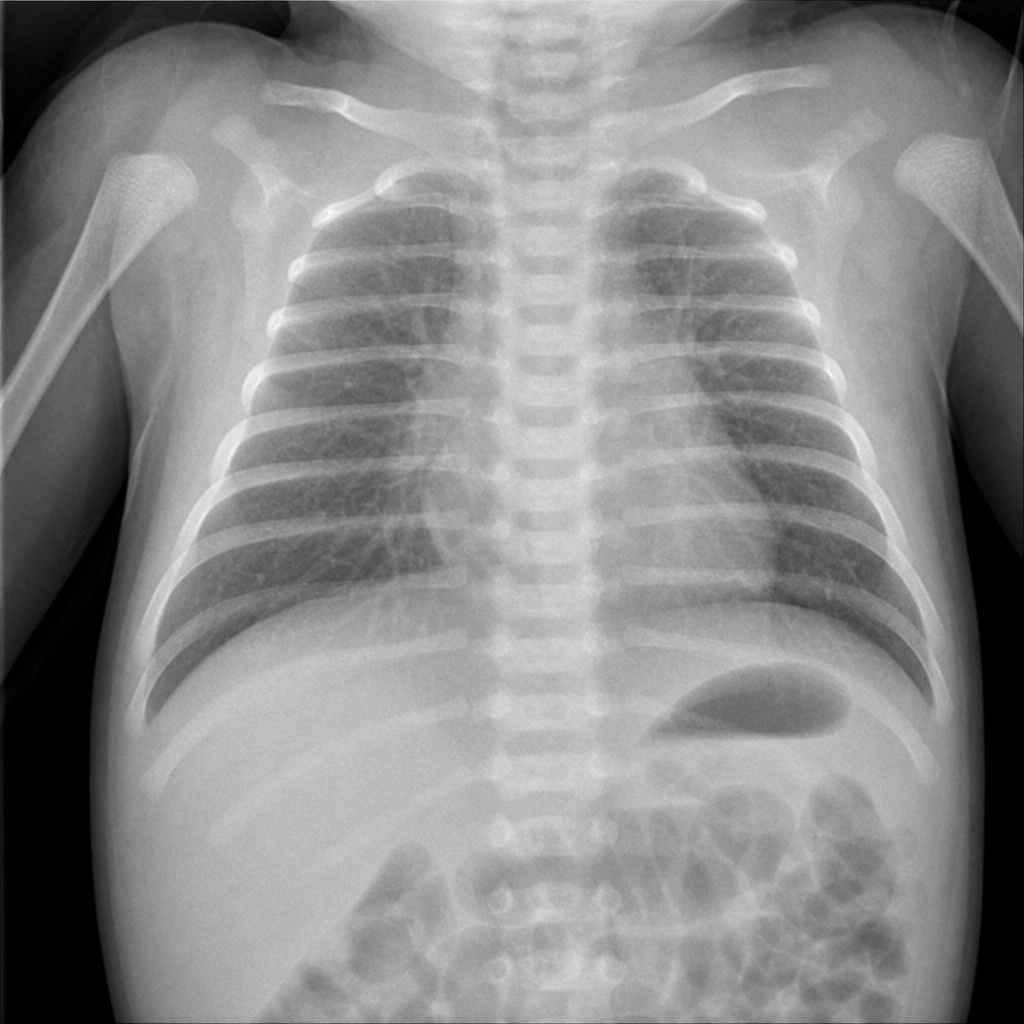
An infant weighing 1600 g is born at 32 weeks' gestation. Initial evaluation was benign, and the infant was transferred to the level 2 nursery for prematurity. At 1 hour of life, the infant is tachypneic with a heart rate of 140 beats per minute, a respiratory rate of 80 breaths per minute, a temperature of 35°C, and a peripheral oxygen saturation of 98%. The lungs are clear with bilateral breath sounds and there is no murmur; the infant is in no distress. The child's chest radiograph is shown. Which of the following is the most appropriate next step in evaluating the infant?
Physiological jaundice in a term baby typically lasts up to how many days?
A diabetic female at 40 weeks of gestation delivered a baby by elective cesarean section. Soon after birth, the baby developed respiratory distress. What is the most likely diagnosis?
Higher incidence of which of the following is seen in the infant of a diabetic mother?
The neonatal period extends up to which point in a newborn's life?
What is the management of a newborn when the mother has active Tuberculosis and is taking Anti-Tuberculosis Treatment (ATT)?
A large for date baby may be due to which of the following conditions?
What is the normal cardiac output of a newborn?
Deficiency of surfactant is seen in which of the following conditions?
In which of the following conditions are steroids NOT indicated for treatment?
Practice by Chapter
Neonatal Resuscitation
Practice Questions
Care of the Normal Newborn
Practice Questions
Prematurity and Low Birth Weight
Practice Questions
Respiratory Distress Syndrome
Practice Questions
Neonatal Jaundice
Practice Questions
Neonatal Sepsis
Practice Questions
Necrotizing Enterocolitis
Practice Questions
Intraventricular Hemorrhage
Practice Questions
Persistent Pulmonary Hypertension
Practice Questions
Perinatal Asphyxia
Practice Questions
Neonatal Seizures
Practice Questions
Congenital Anomalies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app