
Neonatology — MCQs

On this page
All are possible causes of seizures on day 1 of life EXCEPT?
If a mother is HBsAg positive, what management is recommended for the newborn?
Which of the following conditions does NOT typically cross the placenta?
Which of the following is NOT associated with bronchopulmonary dysplasia?
Which one of the following drugs causes QT prolongation in a premature infant?
Pneumatosis intestinalis is most often seen in?
Which statement is not true about cephalohaematoma?
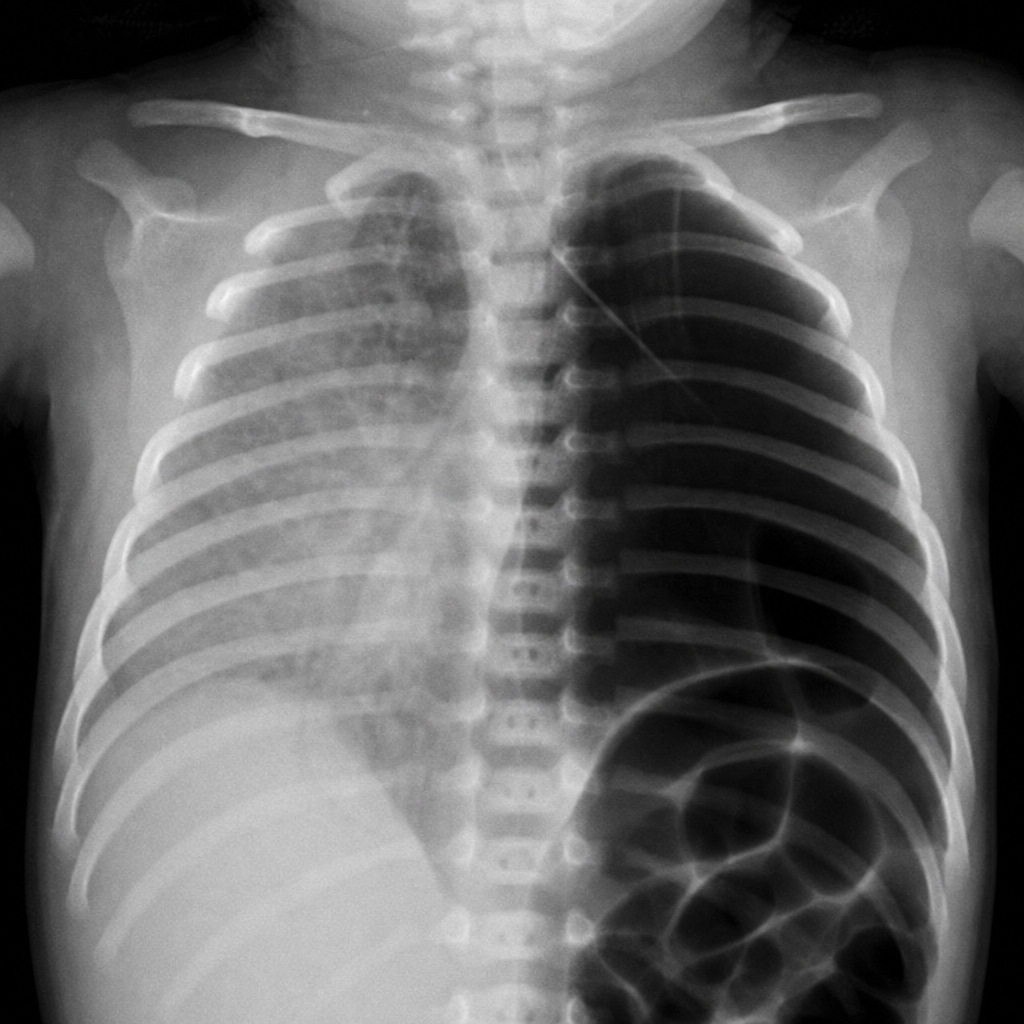
The most likely diagnosis in this child is:
A newborn develops erythematous papular lesions on the face and trunk after 2-3 days of life. A smear of the pustular lesions is prepared. What cells would be seen in the smear?
What are the benefits of the technique shown below, excluding one option?

Practice by Chapter
Neonatal Resuscitation
Practice Questions
Care of the Normal Newborn
Practice Questions
Prematurity and Low Birth Weight
Practice Questions
Respiratory Distress Syndrome
Practice Questions
Neonatal Jaundice
Practice Questions
Neonatal Sepsis
Practice Questions
Necrotizing Enterocolitis
Practice Questions
Intraventricular Hemorrhage
Practice Questions
Persistent Pulmonary Hypertension
Practice Questions
Perinatal Asphyxia
Practice Questions
Neonatal Seizures
Practice Questions
Congenital Anomalies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app