
Neonatal Sepsis — MCQs

Community-acquired neonatal pneumonia: What is the treatment of choice?
A neonate develops sepsis with organism showing CAMP test positive. Likely organism?
Which of the following is not a complication of Congenital Rubella Syndrome (CRS)?
An appropriate single antibiotic for the empiric treatment of presumed bacterial meningitis in a six month old child would be:
A patient with a fever presents with a heart rate of 120 beats per minute and a respiratory rate of 30 breaths per minute. What does this indicate?
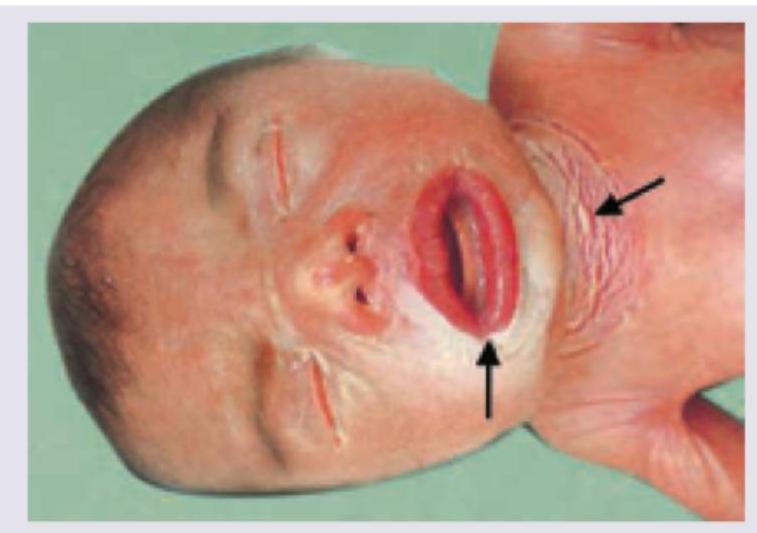
A neonate presents with the condition shown in the image below. This condition has all of the following features EXCEPT:
What is the most common cause of pneumonia in early onset sepsis in neonates?
A neonate who is febrile, presents with features of encephalitis. On examination, the baby is found to have vesicular skin lesions. Most probable causative organism is:
A term neonate, with a birth weight of 2700 g, who is otherwise well, and is exclusively breastfed, presents for routine evaluation. His total serum bilirubin is found to be 14mg/dl on day 5. What is the management?
Erythematous blotchy rash is seen on the abdomen, trunk, and face of a 3-day-old child along with yellowish papules. The child appears well. What is the appropriate management?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app