
Neonatal Seizures — MCQs

Which of the following statements is MOST accurate regarding neonatal sepsis?
A preterm infant with poor respiration at birth starts throwing seizures at 10 hours after birth. Antiepileptic of choice shall be:
All are primary generalised seizures except
Which of the following electrolyte abnormalities is a cause of status epilepticus in a child?
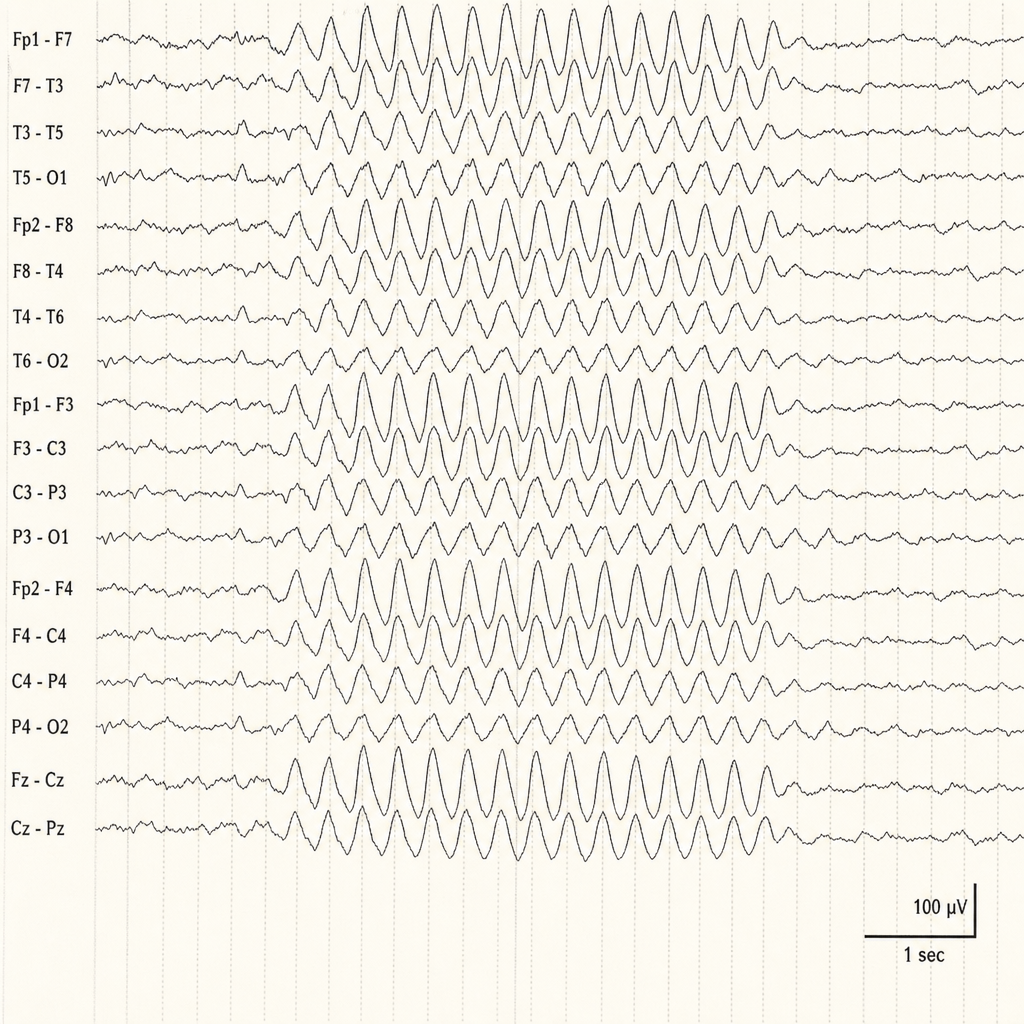
A 7 years old girl with falling grades and complaints by teacher that she is inattentive in class to her parents and has bad school performance. On hyperventilation her symptoms increased and showed the following EEG findings. Diagnosis is (graph is given):
A sick intubated neonate is having bilateral jerk of both right and left upper limbs with some occasional twitching of neck as well. Likely type of seizures:
The recommended ambient temperature for NICU is
A term neonate, with a birth weight of 2700 g, who is otherwise well, and is exclusively breastfed, presents for routine evaluation. His total serum bilirubin is found to be 14mg/dl on day 5. What is the management?
Most common cause of convulsion on the first day of life in a newborn is:
Which of the following is NOT included in the resuscitation of a neonate with HR < 60/min?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app