
Intraventricular Hemorrhage — MCQs

A 3-4 month old baby with heart rate 250/min, QRS complex less than 0.07 sec and no P wave, Diagnosis will be :
Most common cause of interventricular bleed is?
Earliest clinical sign of raised intracranial pressure is:
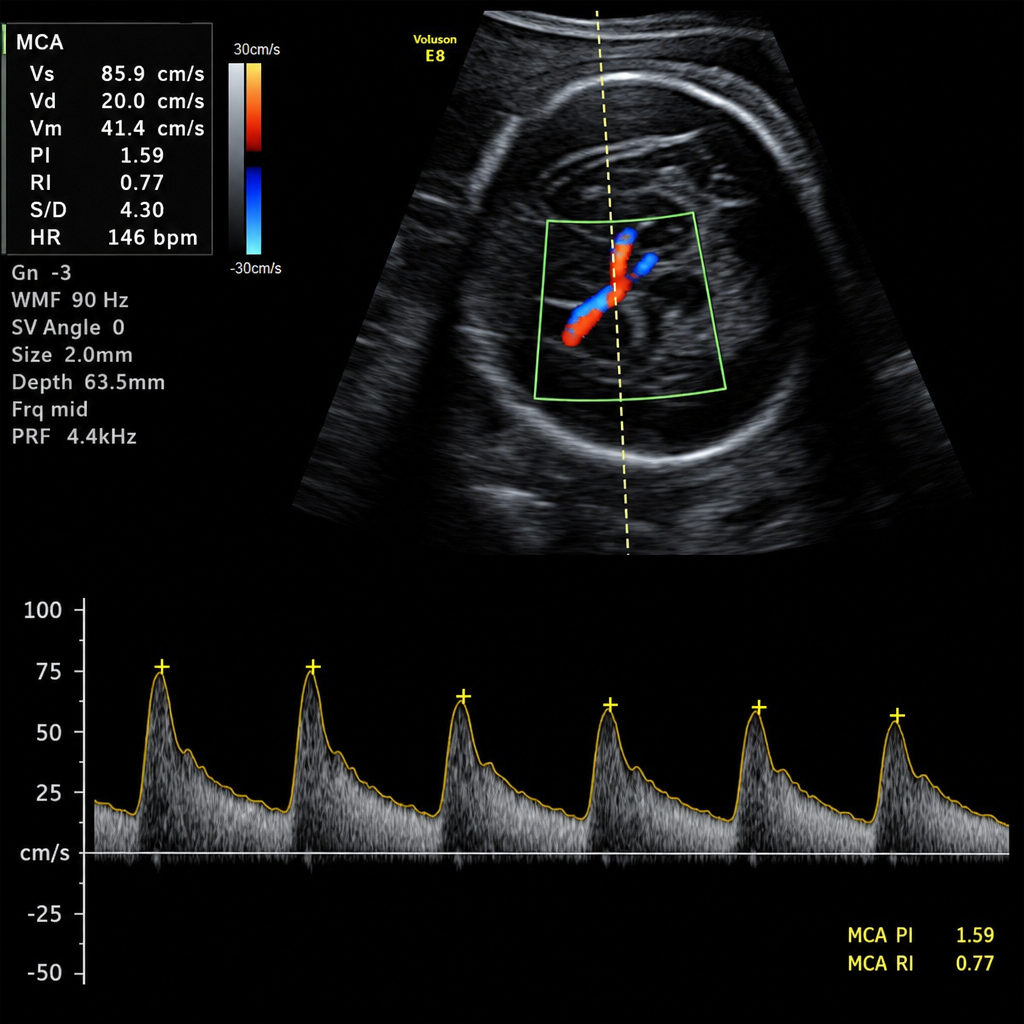
A 28-week pregnant female presents with fetal distress on examination, and the MCA Doppler study is as follows. What should be the next step in management?
Which of the following medications is contraindicated in head trauma patients?
What is the preferred management for patent ductus arteriosus (PDA) in a preterm infant?
Which condition is associated with exclusively fetal blood loss?
A child with moderate to severe head injury is admitted in PICU. First line treatments are all except:
Following are the features of raised intracranial tension except -
A newborn presents with subconjunctival hemorrhage. The treatment is
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app