
Infectious Diseases — MCQs

On this page
A previously healthy child develops bacterial meningitis. Assuming no specific contraindications, which of the following is the drug of choice?
A 3-year-old child presents with fever, malaise, and oral ulcers, making swallowing difficult. What is the most likely diagnosis?
Which of the following is TRUE about measles, EXCEPT?
What is the most common complication of mumps?
Which of the following conditions does NOT typically present with a maculopapular rash?
Which of the following symptoms is NOT suggestive of Scarlet fever?
Which of the following statements regarding typhoid in children is false?
In rubella syndrome, all are seen except?
What management is indicated for an infant born to an HIV-positive mother?
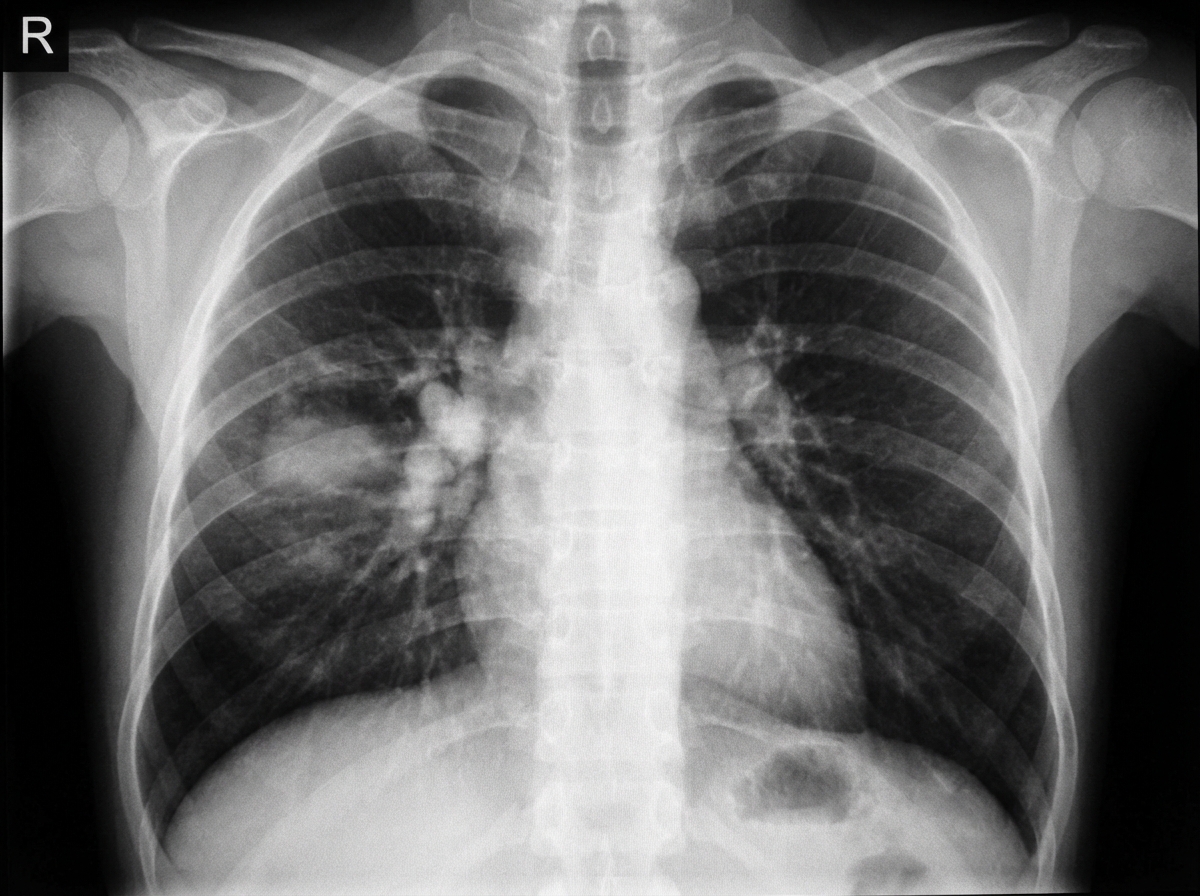
A 4-year-old child presented with cough persisting for 1 month and low-grade fever. There was a history of contact with TB. What is the chest X-ray suggestive of?
Practice by Chapter
Vaccine-Preventable Diseases
Practice Questions
Immunization Schedule
Practice Questions
Common Childhood Infections
Practice Questions
Pediatric HIV
Practice Questions
Congenital Infections
Practice Questions
Fever in Infants and Children
Practice Questions
Meningitis and Encephalitis
Practice Questions
Respiratory Tract Infections
Practice Questions
Gastrointestinal Infections
Practice Questions
Parasitic Infections
Practice Questions
Tuberculosis in Children
Practice Questions
Opportunistic Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app