
Infectious Diseases — MCQs

On this page
Which of the following are the features of Rubella? 1. Rashes appear within 24 hours of onset of symptoms 2. Incubation period is 2 – 3 weeks 3. False membrane is formed in throat 4. Post auricular lymph nodes enlarge Select the correct answer using the code given below:
With reference to mumps, consider the following statements: 1. The average age of incidence of mumps is higher than that of measles and chicken pox. 2. The mumps disease tends to be more severe in adults than in children. Which of the statements given above is/are correct?
Which of the following is a contraindication for BCG vaccination in a newborn?
Which one of the following is the recommended site for immunization with hepatitis B vaccine in young children for ensuring reliable absorption?
Which statement about congenital syphilis is FALSE?
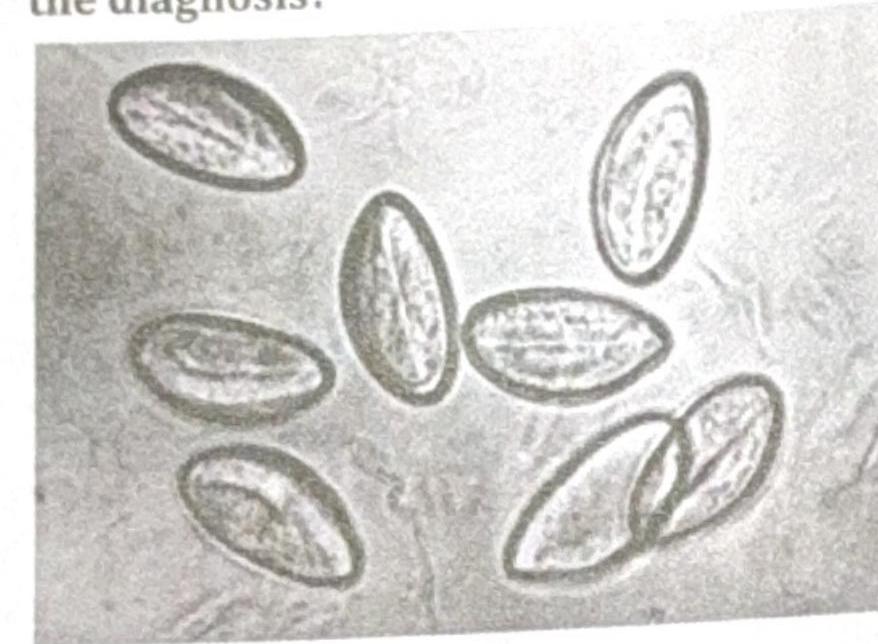
A child presented with perianal itching. The swab specimen is shown in the image. What is the diagnosis?
A 10 week old child comes for vaccination, with previous history of inconsolable cry & fever after getting vaccinated at 6 weeks. What should be done next?
A 10-week-old baby came for vaccination. The baby had a previous history of inconsolable crying and fever (40°C) after vaccination at 6 weeks. What should be given now?
A child presenting with the following appearance is at risk of developing?

A child presents with fever and vesicular lesions on the upper limb and the lower limb. Neck stiffness was present. Similar lesions were present on the palms, soles, and oral cavity. CSF analysis revealed normal glucose levels and elevated lymphocytes and protein. What is the most likely diagnosis?
Practice by Chapter
Vaccine-Preventable Diseases
Practice Questions
Immunization Schedule
Practice Questions
Common Childhood Infections
Practice Questions
Pediatric HIV
Practice Questions
Congenital Infections
Practice Questions
Fever in Infants and Children
Practice Questions
Meningitis and Encephalitis
Practice Questions
Respiratory Tract Infections
Practice Questions
Gastrointestinal Infections
Practice Questions
Parasitic Infections
Practice Questions
Tuberculosis in Children
Practice Questions
Opportunistic Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app