
Infectious Diseases — MCQs

On this page
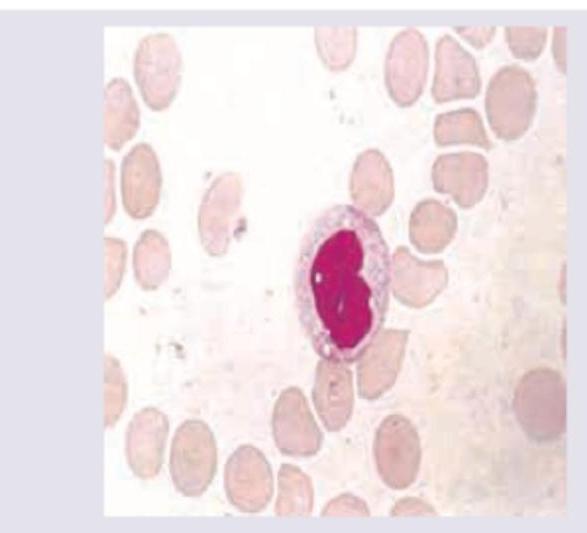
A 12-year-old child presents with fever, sore throat for 3 days and posterior cervical lymphadenopathy. Peripheral smear was performed. Diagnosis is?
A child is brought to your OPD with rashes as shown below along with fever. Diagnosis is:

Which of the following statements are correct regarding vaccination routes for children? I. Hepatitis B vaccine given in deltoid region has reduced efficacy II. Two vaccines may be given in the same thigh, but separated by 1 inch III. Separate sites are used when administering a vaccine and an immunoglobulin IV. Two intramuscular vaccines should never be given on the same day Select the answer using the code given below:
In a child aged 3-12 years with an ear problem, which one of these situations merits urgent referral to hospital?
Which of the following statements are correct about oral rotavirus vaccines? I. The storage should be at 2-8°C II. The vaccine should be used within 2 hours of reconstitution or opening III. Past history of intussusception is a contraindication IV. The vaccine can be given if the baby has ongoing diarrhoea Select the answer using the code given below :
All cases of severe measles and all cases of measles in areas with high case fatality rate need to be treated with which of the following vitamins?
In measles, when do the Koplik's spots appear?
Varicella-Zoster Immunoglobulin (VZIG) is NOT recommended for which of the exposed susceptible individuals?
The classical triad of congenital defects in Congenital Rubella Syndrome include which of the following? 1. Hydrocephalus 2. Deafness 3. Cardiac malformations 4. Cataract
Which of the following are the features of Rubella? 1. Rashes appear within 24 hours of onset of symptoms 2. Incubation period is 2 – 3 weeks 3. False membrane is formed in throat 4. Post auricular lymph nodes enlarge Select the correct answer using the code given below:
Practice by Chapter
Vaccine-Preventable Diseases
Practice Questions
Immunization Schedule
Practice Questions
Common Childhood Infections
Practice Questions
Pediatric HIV
Practice Questions
Congenital Infections
Practice Questions
Fever in Infants and Children
Practice Questions
Meningitis and Encephalitis
Practice Questions
Respiratory Tract Infections
Practice Questions
Gastrointestinal Infections
Practice Questions
Parasitic Infections
Practice Questions
Tuberculosis in Children
Practice Questions
Opportunistic Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app