
Infectious Diseases — MCQs

On this page
An HIV-positive mother with a viral load of 1200 copies/mL delivers a baby. What is the most appropriate antiretroviral prophylaxis for the newborn?
A 6-week-old child with tuberous sclerosis, whose infantile spasms are controlled and neurologic condition is stable, is on vigabatrin and has been brought for vaccination. Birth vaccines were already received. Which of the following pertussis-containing vaccine formulation is least likely to cause fever or seizures in this child?

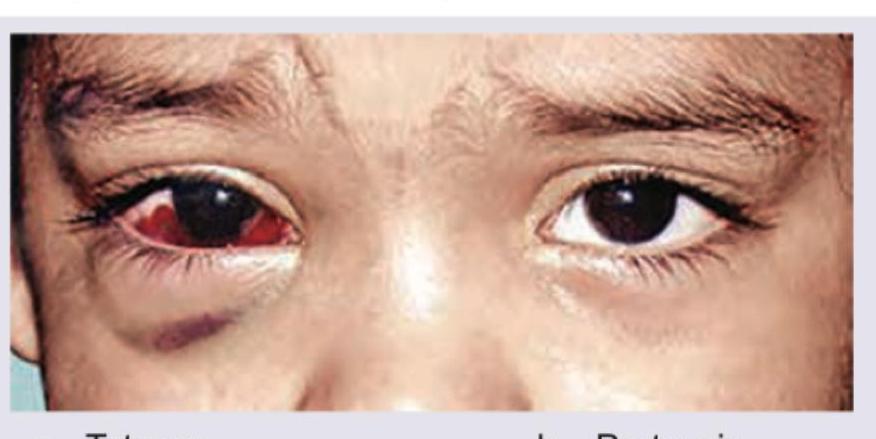
A child presents with a 2-week history of paroxysmal coughing fits followed by an inspiratory whoop and post-tussive vomiting. The ocular findings shown in the image below are noted on examination. Identify the most likely underlying illness:
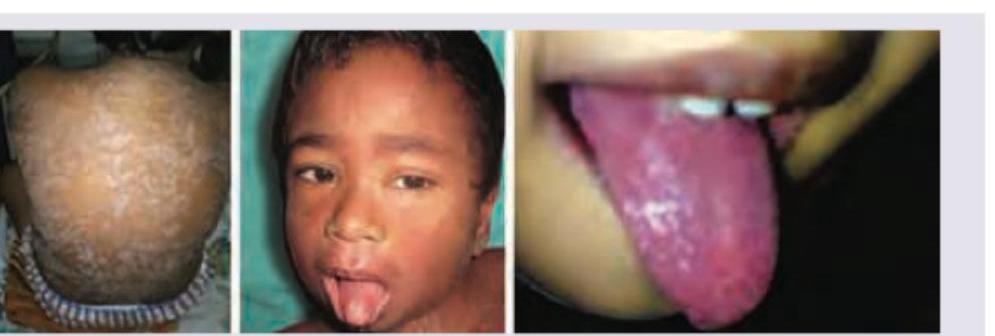
A child presents with high fever, cough, coryza, conjunctivitis, and Koplik spots, followed by a maculopapular rash that started on the face and behind the ears and spread cephalocaudally. Identify the diagnosis:

Which is the most common complication of this rash?

A 5-year-old child in a village went for open air defecation when he was attacked by a dog. He has been admitted in your hospital, all are correct about the condition except: (Recent NEET Pattern 2016-17)

A 6-year-old child from Kashmir is brought to New Delhi hospital in delirious condition with history of high grade fever for last 10 days. He is nonresponsive to commands and blanching rash is noted all over the body especially soles and palms. Per abdomen examination shows splenohepatomegaly. Blood culture was sterile after 48 hours of incubation, WeilFelix reaction shows increasing antibody titer and complement fixation test was positive. Which is the best treatment for the patient?
A 6-year-old child from Kashmir is brought to New Delhi hospital in a delirious condition with history of high grade fever for last 10 days. He is nonresponsive to commands and blanching rash is noted all over the body especially soles and palms. Per abdomen examination shows splenohepatomegaly. Probable diagnosis is:

A 4-year-old child presents with fever for 4 days with decreased oral intake. On examination a rough textured rash on trunk is seen which blanches on pressure. Later the rash fades and desquamation occurs. All are true about the condition except:
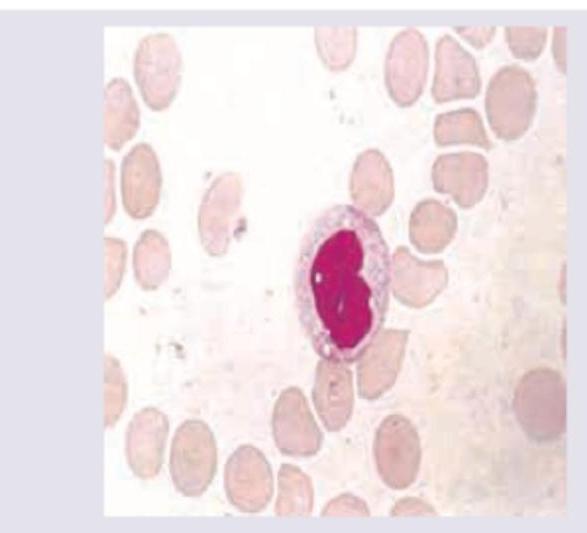
A 12-year-old child presents with fever, sore throat for 3 days and posterior cervical lymphadenopathy. Peripheral smear was performed. Diagnosis is?
Practice by Chapter
Vaccine-Preventable Diseases
Practice Questions
Immunization Schedule
Practice Questions
Common Childhood Infections
Practice Questions
Pediatric HIV
Practice Questions
Congenital Infections
Practice Questions
Fever in Infants and Children
Practice Questions
Meningitis and Encephalitis
Practice Questions
Respiratory Tract Infections
Practice Questions
Gastrointestinal Infections
Practice Questions
Parasitic Infections
Practice Questions
Tuberculosis in Children
Practice Questions
Opportunistic Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app