
Infectious Diseases — MCQs

On this page
What is helpful in a child with severe falciparum malaria with high parasitemia?
Excessive crying is a known side effect following which vaccination?
A 9-year-old girl presents with a 2-day history of sore throat. Physical examination reveals pharyngeal erythema with yellowish exudates over swollen palatine tonsils. A Gram stain of the exudate shows gram-positive cocci in chains. She is treated with penicillin. What is the most likely complication prevented by prompt treatment?
DPT vaccine is contraindicated in which of the following conditions?
A 10-year-old child presents to the OPD with fever, neck rigidity, convulsions, and signs of meningeal irritation. Cerebrospinal fluid (CSF) examination shows normal glucose, slightly elevated proteins, and appears clear on gross examination. What is the most probable diagnosis?
What is the most common complication of measles in children?
Which of the following is true about cerebral malaria in children?
Subdural effusions in association with acute bacterial meningitis are:
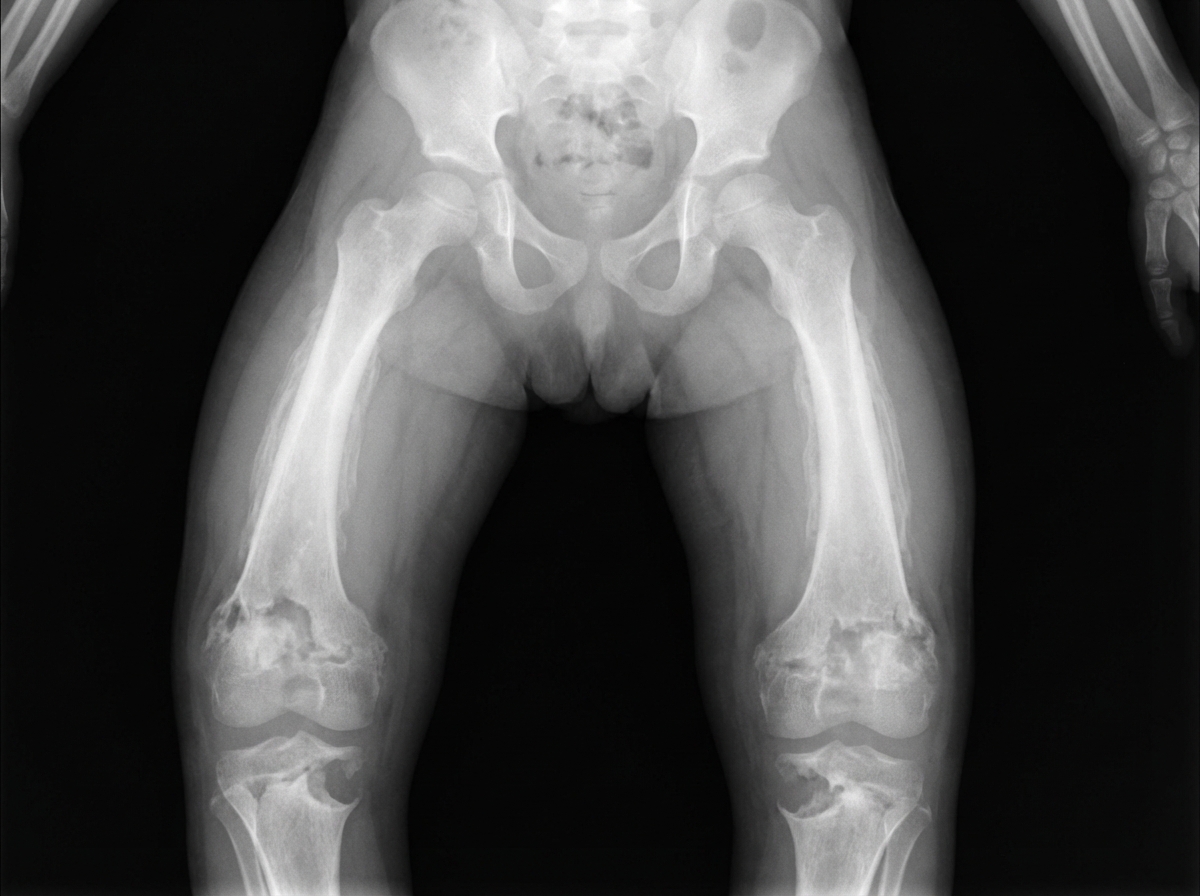
A radiograph of a child is shown below. What is the most likely diagnosis?
A 2-year-old boy presents in late summer with a 2-day history of painful, ulcerative lesions of the mouth and a 1-day history of fever up to 103°F. He refuses to eat. On examination, he is irritable with a temperature of 102°F and has numerous erythematous, ulcerative lesions on the buccal mucosa and tongue. What is the most likely diagnosis?
Practice by Chapter
Vaccine-Preventable Diseases
Practice Questions
Immunization Schedule
Practice Questions
Common Childhood Infections
Practice Questions
Pediatric HIV
Practice Questions
Congenital Infections
Practice Questions
Fever in Infants and Children
Practice Questions
Meningitis and Encephalitis
Practice Questions
Respiratory Tract Infections
Practice Questions
Gastrointestinal Infections
Practice Questions
Parasitic Infections
Practice Questions
Tuberculosis in Children
Practice Questions
Opportunistic Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app