
Infectious Diseases — MCQs

On this page
An unimmunized child presents with signs suggestive of diphtheria. Which type of diphtheria would suggest the worst prognosis?
Which of the following organisms causes pneumatocele in children in association with pneumonia?
A baby is born to a mother with AIDS. Which of the following statements is true regarding the infant, except?
A 4-month-old infant presents with failure to thrive, progressive muscular weakness, and poor head control. The mother states that she feeds the baby soy-based formula sweetened with honey. Which organism is most likely responsible for these symptoms?
An 18-month-old baby with poor feeding and fever for 3 days presents with lower limb weakness. On examination, the baby is lethargic, has abnormal movement of the lower limbs, and the anterior fontanelle is bulging. What is the diagnosis?
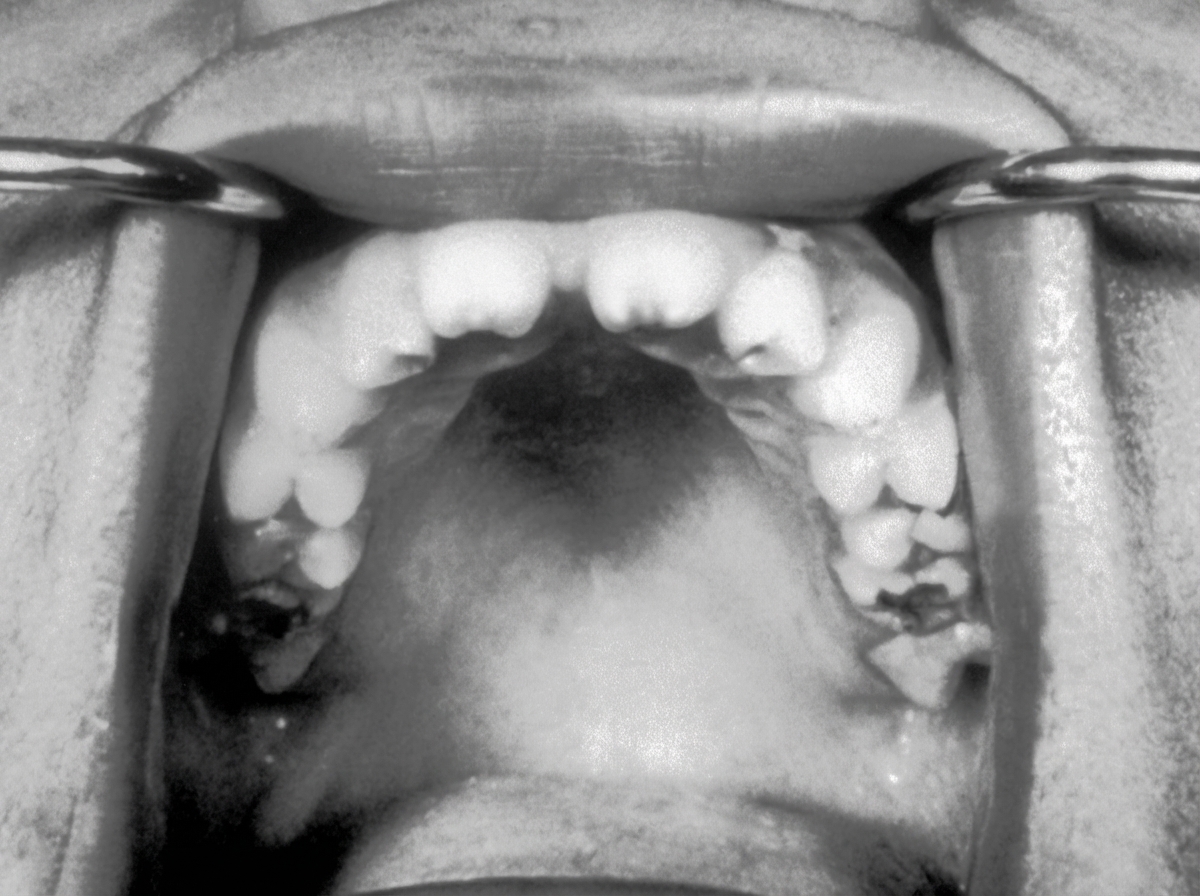
The teeth abnormality shown in the image is seen in which of the following diseases?
Which of the following is true about erythema infectiosum?
Hutchinson teeth are a characteristic feature of which condition?
A 12-year-old child presents with fever and cervical lymphadenopathy for the last 36 hours. Oral examination shows a grey membrane on the right tonsil. What is the primary treatment?
A 6-year-old child develops a sore throat with high-grade fever. On examination, there was tender bilateral cervical adenopathy. Considering the findings, which of the following complications or outcomes will NOT be prevented or reduced by the administration of antibiotics?
Practice by Chapter
Vaccine-Preventable Diseases
Practice Questions
Immunization Schedule
Practice Questions
Common Childhood Infections
Practice Questions
Pediatric HIV
Practice Questions
Congenital Infections
Practice Questions
Fever in Infants and Children
Practice Questions
Meningitis and Encephalitis
Practice Questions
Respiratory Tract Infections
Practice Questions
Gastrointestinal Infections
Practice Questions
Parasitic Infections
Practice Questions
Tuberculosis in Children
Practice Questions
Opportunistic Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app