
Immunology and Allergies — MCQs

On this page
Abdominal pain in Henoch-Schonlein purpura is most commonly due to which of the following mechanisms?
A child presents with recurrent Staphylococcus infections. Laboratory examination shows very low levels of immunoglobulins (G, A, M, E), and a low quantity of B cells. There is a normal reaction to environmental antigens on the skin. What is the most likely diagnosis?
A 5-year-old short stature boy presented with fever and weight loss for 6 weeks. He has been admitted previously for 4 episodes of pneumonia in last year. On examination neck lymph nodes were enlarged and reddish macules were noticed on the face and forehead. Lymph node biopsy shows Hodgkin's disease. What is the diagnosis?
A 7-year-old boy presents with palpable non-blanching rash starting 3 days back from the ankles and involves lower limbs and buttocks. He had viral URTI previously. BP is normal and KFT is normal. What is the diagnosis?
A child presents with low grade fever for 5 days, joint pain in large joints and palpable purpuric rash on lower extremities and buttocks. The most probable diagnosis is:
A 6-year-old child with abdominal pain and a rash is shown. Comment on the diagnosis?
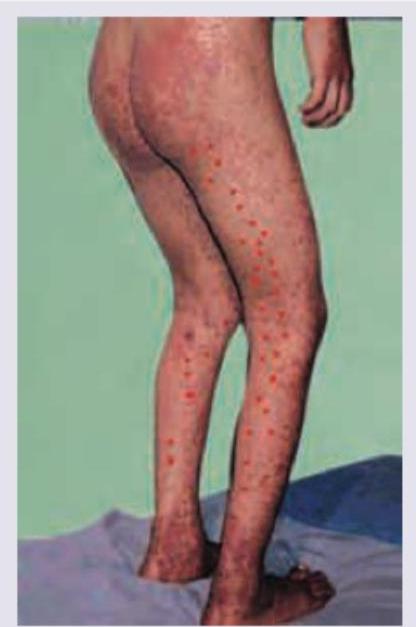
A child presents with blotchy rash on legs, back and buttocks. All are true about the condition except:
Which of the following are causes of secondary immunodeficiency in children? I. Diphenylhydantoin II. Severe malnutrition III. Post-varicella state IV. Nephrotic syndrome Select the correct answer using the code given below :
Eight months old child had history of unusual crying and convulsions following previous vaccination after BCG, DPT & OPV ( first dose), and Hepatitis B. Now parents have brought child for next doses of vaccination. Which vaccine is contraindicated in this situation?
A 10-year-old boy presents with fever, joint pain, and a lesion over his hand, as seen in the image below. Which of the following is the clinical finding, and what is the likely diagnosis?

Practice by Chapter
Development of Immune System
Practice Questions
Primary Immunodeficiency Disorders
Practice Questions
Secondary Immunodeficiency Disorders
Practice Questions
Allergic Rhinitis
Practice Questions
Asthma in Children
Practice Questions
Atopic Dermatitis
Practice Questions
Food Allergies
Practice Questions
Drug Allergies
Practice Questions
Anaphylaxis
Practice Questions
Urticaria and Angioedema
Practice Questions
Autoimmune Disorders
Practice Questions
Immunotherapy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app