
Growth and Development — MCQs

On this page
All are common in Down syndrome, except?
Which of the following statements about fragile X syndrome is FALSE?
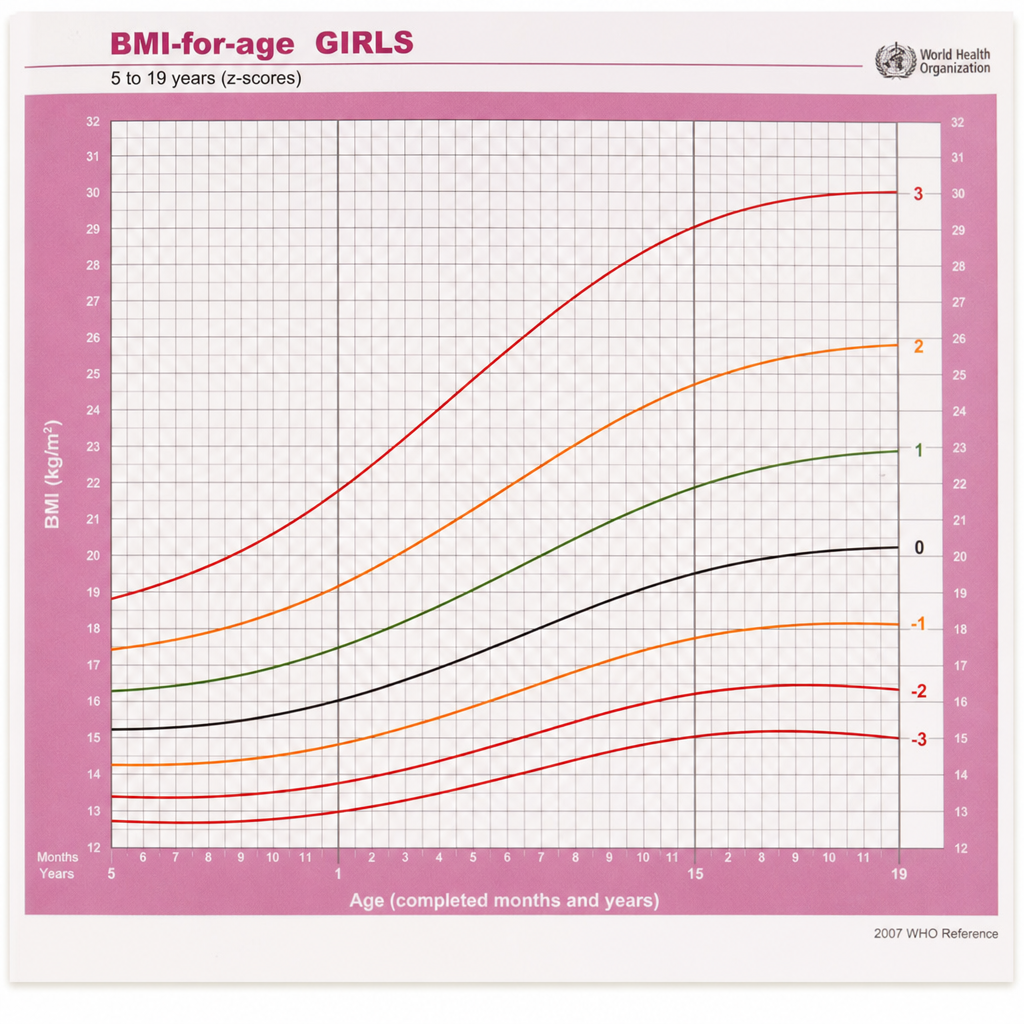
Ignoring the superimposed arrows, which statement best describes the growth chart shown?
Which of the following developmental milestones is achieved first?
A 6-year-old child presents with mild mental retardation, superiority in musical aptitude, and social amiability. The child has a distinctive but subtle physical appearance described as 'elfin appearance'. Which of the following best describes the child's condition?
What is a developmental milestone typically achieved by a 1.5-year-old child?
A boy can grasp a rattle and has recently learned to transfer objects from one hand to another. What developmental milestone can he likely achieve next?
Which of the following is NOT a feature of Prader-Willi syndrome?
A child begins to sit with support, is able to transfer objects from one hand to another, and speaks monosyllabic babbles at what age?
A child is able to say sentences of 6 words. What is the likely age of this child?
Practice by Chapter
Normal Growth Parameters
Practice Questions
Developmental Milestones
Practice Questions
Puberty and Adolescent Development
Practice Questions
Growth Disorders
Practice Questions
Failure to Thrive
Practice Questions
Developmental Screening and Assessment
Practice Questions
Developmental Delays
Practice Questions
Growth Charts and Monitoring
Practice Questions
Short Stature
Practice Questions
Tall Stature
Practice Questions
Precocious and Delayed Puberty
Practice Questions
Psychosocial Development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app