
Growth and Development — MCQs

On this page
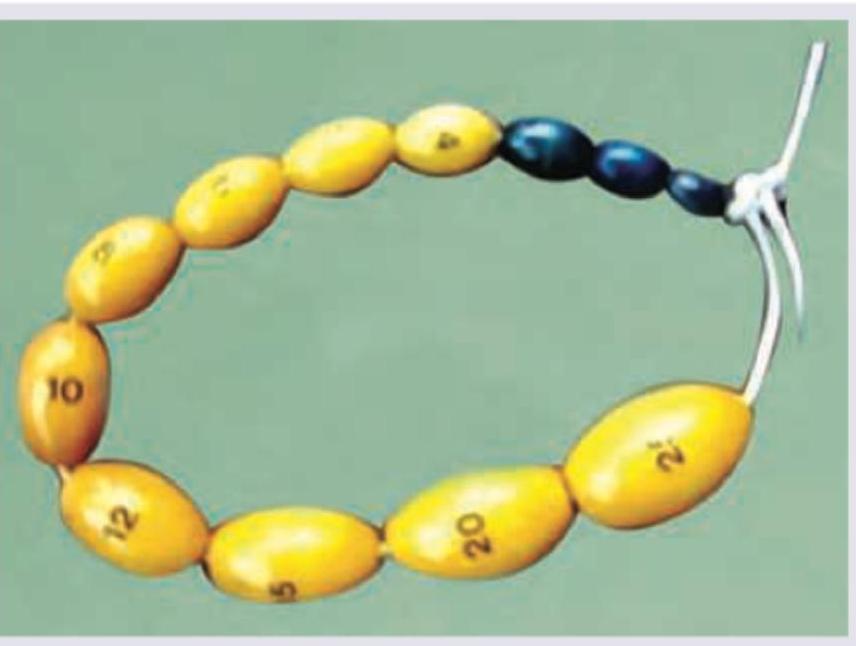
Which is true about the instrument shown?
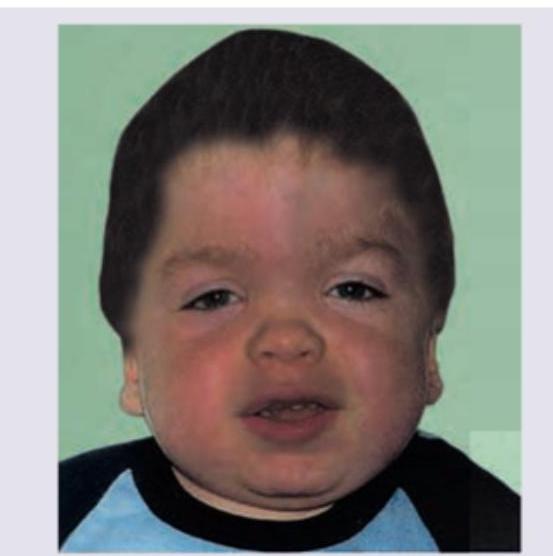
What is the diagnosis of this child with short stature and corneal opacity?
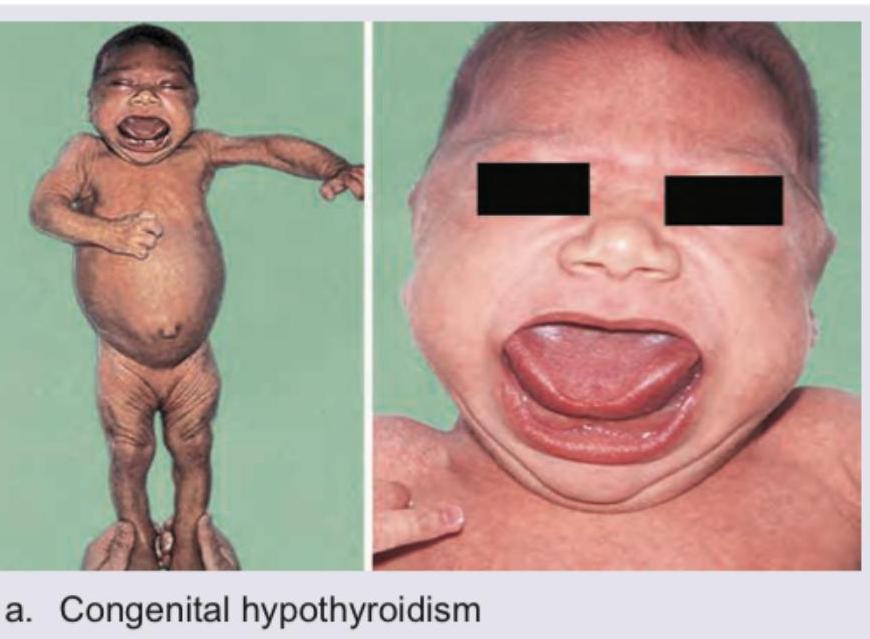
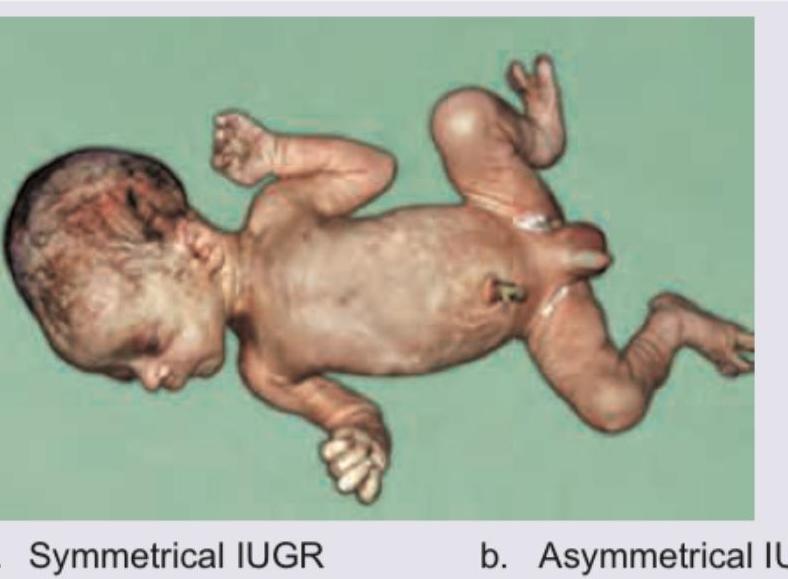
A newborn male infant presents with the findings shown in the image. The clinical diagnosis is?

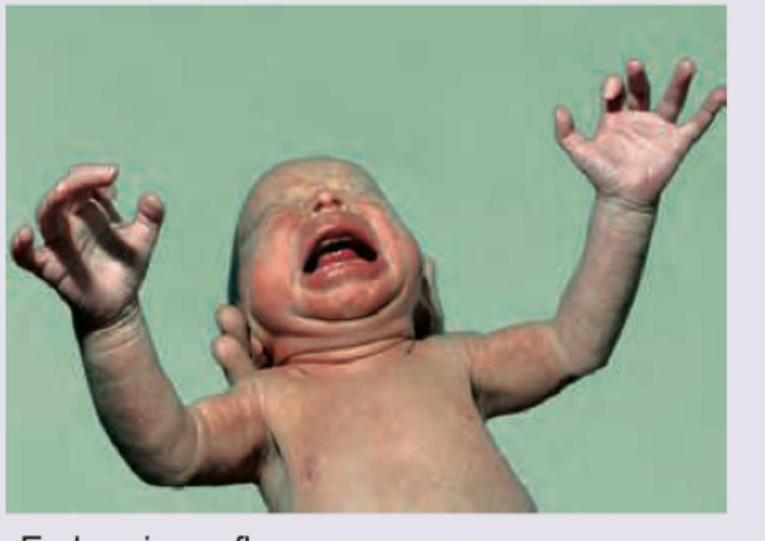
A newborn presents with macrosomia, plethoric appearance, and generalized edema. The image shows:

Comment on the diagnosis of the child:
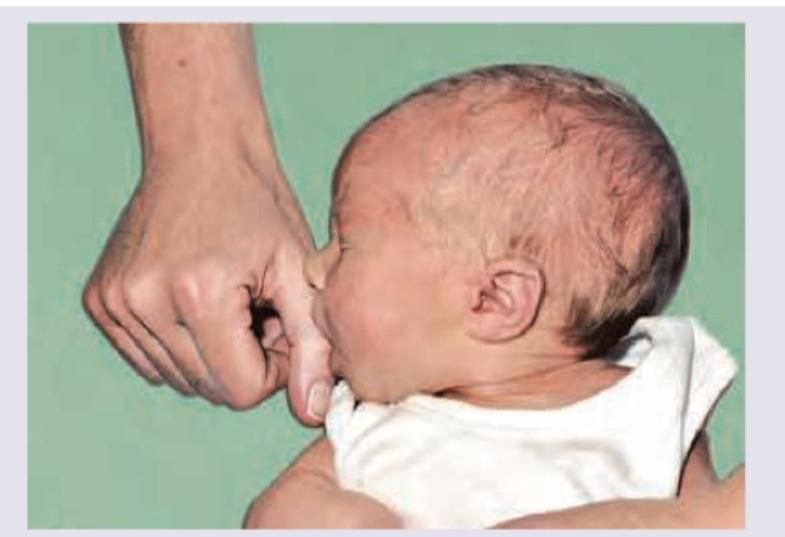
All are true about this reflex except:
The reflex shown below disappears by what age?
One-year-old child with refractory epilepsy. Which is incorrect about the child in picture given below?

The image shows:
The image shows presence of:

Practice by Chapter
Normal Growth Parameters
Practice Questions
Developmental Milestones
Practice Questions
Puberty and Adolescent Development
Practice Questions
Growth Disorders
Practice Questions
Failure to Thrive
Practice Questions
Developmental Screening and Assessment
Practice Questions
Developmental Delays
Practice Questions
Growth Charts and Monitoring
Practice Questions
Short Stature
Practice Questions
Tall Stature
Practice Questions
Precocious and Delayed Puberty
Practice Questions
Psychosocial Development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app